Li Huan-Jun, Chen Yu-Tong, Yuan Shu-Qiang
Department of Medical Oncology, Dongguan General Hospital, Dongguan Department of Medical Oncology, Sun Yat-Sen University Cancer Center State Key Laboratory of Oncology in South China Collaborative Innovation Center for Cancer Medicine Department of Gastric and Pancreatic Surgery, Sun Yat-Sen University Cancer Center, Guangzhou, China.
Medicine (Baltimore). 2018 Aug;97(34):e12094. doi: 10.1097/MD.0000000000012094.
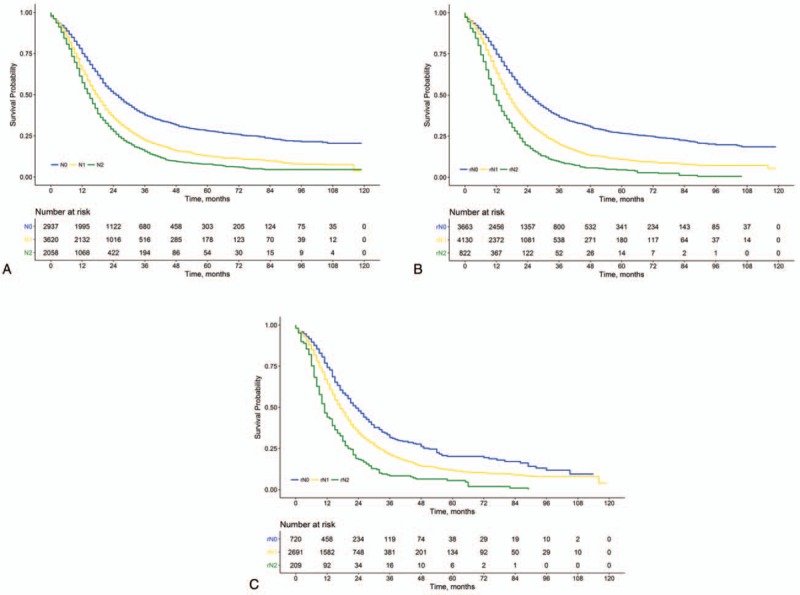
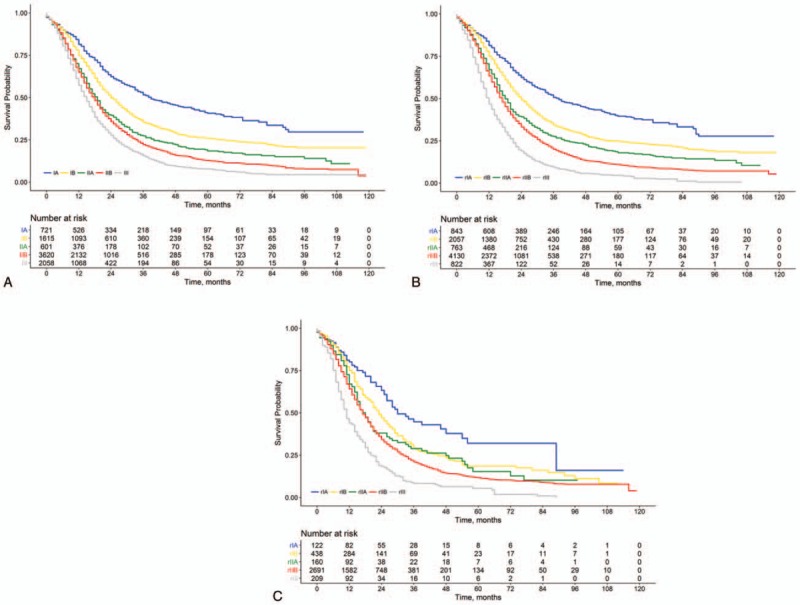
The recently launched 8th edition of the American Joint Committee on Cancer (AJCC) staging scheme for pancreatic ductal adenocarcinoma (PDAC) did not account for the impact of the total examined lymph node count on prognostic accuracy. In this population-based cohort study, we proposed a modified AJCC staging scheme by incorporating a lymph node ratio (LNR)-based N classification for patients with resectable PDAC.We analyzed 8615 patients with resectable PDAC from the Surveillance, Epidemiology, and End Results database between 2004 and 2013. The optimal cut-off points for LNR were identified by recursive partitioning, and an LNR-based N classification was designed accordingly.The LNR-based N classification could further stratify patients with the 8th AJCC N1 and N2 disease into subgroups with significantly different overall survival (P < .001 for both). By replacing the 8th AJCC N classification with the corresponding LNR-based N classification, we further proposed a modified AJCC staging scheme. The modified AJCC staging outperformed the 8th AJCC staging in terms of the discriminatory capacity measured by the concordance index and Akaike information criterion, and the prognostic homogeneity assessed by using the likelihood ratio chi-squared test and stratified survival analysis.Replacing the 8th AJCC N classification with the LNR-based N classification can improve the prognostic performance of the 8th AJCC staging scheme for PDAC.
美国癌症联合委员会(AJCC)最近发布的第八版胰腺导管腺癌(PDAC)分期方案未考虑检查的淋巴结总数对预后准确性的影响。在这项基于人群的队列研究中,我们通过纳入基于淋巴结比率(LNR)的N分类,为可切除的PDAC患者提出了一种改良的AJCC分期方案。我们分析了2004年至2013年间监测、流行病学和最终结果数据库中的8615例可切除的PDAC患者。通过递归划分确定LNR的最佳截断点,并据此设计基于LNR的N分类。基于LNR的N分类可将第八版AJCC N1和N2期疾病患者进一步分层为总生存期显著不同的亚组(两者P均<0.001)。通过用相应的基于LNR的N分类取代第八版AJCC N分类,我们进一步提出了一种改良的AJCC分期方案。在一致性指数和赤池信息准则衡量的区分能力以及使用似然比卡方检验和分层生存分析评估的预后同质性方面,改良的AJCC分期优于第八版AJCC分期。用基于LNR的N分类取代第八版AJCC N分类可以提高第八版AJCC PDAC分期方案的预后性能。