Cleveland Clinic Foundation Lerner College of Medicine of Case Western Reserve University, Cleveland, OH, USA.
Analysis Group, Inc., 1000 De La Gauchetière Ouest, Suite 1200, Montreal, QC, H3B 4W5, Canada.
Cardiovasc Diabetol. 2018 Aug 24;17(1):118. doi: 10.1186/s12933-018-0759-z.
There exist several predictive risk models for cardiovascular disease (CVD), including some developed specifically for patients with type 2 diabetes mellitus (T2DM). However, the models developed for a diabetic population are based on information derived from medical records or laboratory results, which are not typically available to entities like payers or quality of care organizations. The objective of this study is to develop and validate models predicting the risk of cardiovascular events in patients with T2DM based on medical insurance claims data.
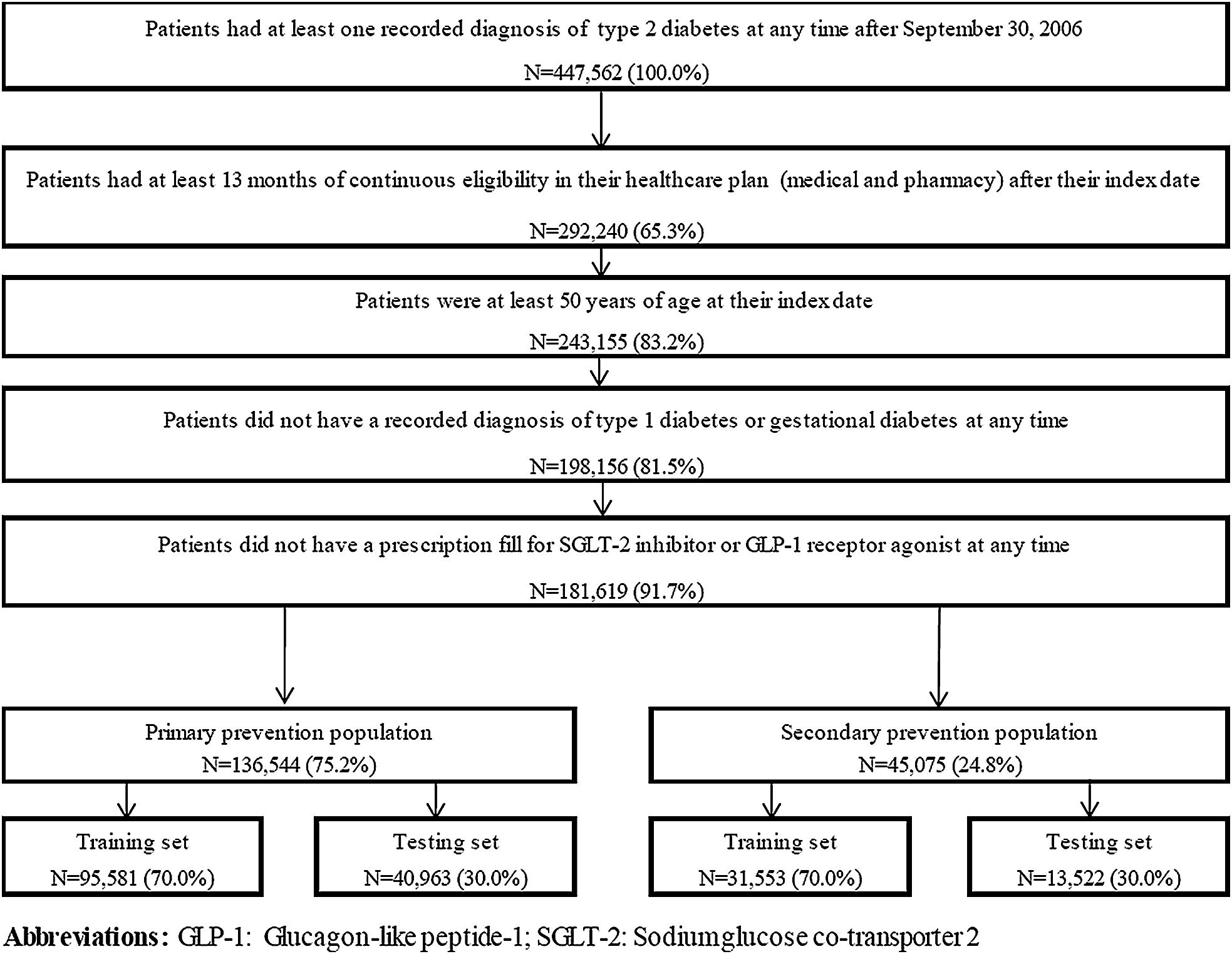
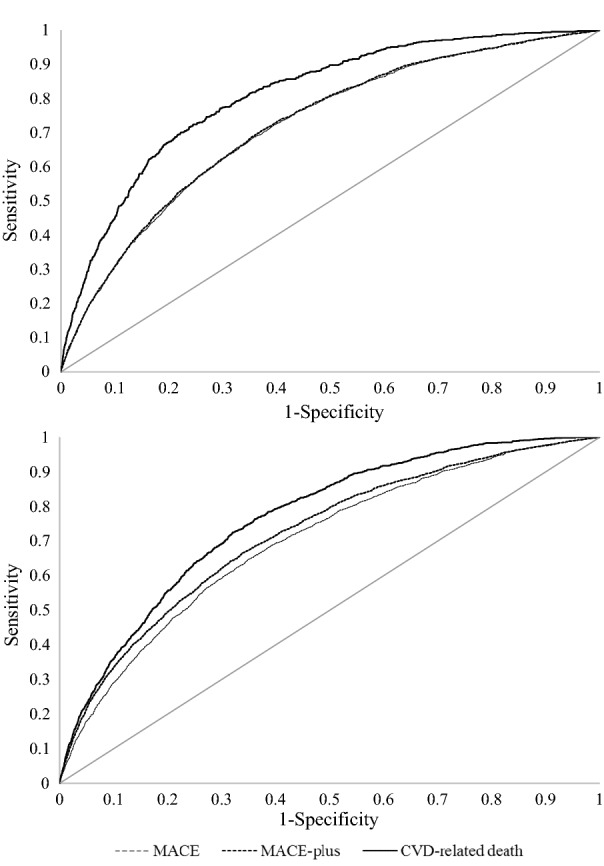
Patients with T2DM aged 50 years or older were identified from the Optum™ Integrated Real World Evidence Electronic Health Records and Claims de-identified database (10/01/2006-09/30/2016). Risk factors were assessed over a 12-month baseline period and cardiovascular events were monitored from the end of the baseline period until end of data availability, continuous enrollment, or death. Risk models were developed using logistic regressions separately for patients with and without prior CVD, and for each outcome: (1) major adverse cardiovascular events (MACE; i.e., non-fatal myocardial infarction, non-fatal stroke, CVD-related death); (2) any MACE, hospitalization for unstable angina, or hospitalization for congestive heart failure; (3) CVD-related death. Models were developed and validated on 70% and 30% of the sample, respectively. Model performance was assessed using C-statistics.
A total of 181,619 patients were identified, including 136,544 (75.2%) without prior CVD and 45,075 (24.8%) with a history of CVD. Age, diabetes-related hospitalizations, prior CVD diagnoses and chronic pulmonary disease were the most important predictors across all models. C-statistics ranged from 0.70 to 0.81, indicating that the models performed well. The additional inclusion of risk factors derived from pharmacy claims (e.g., use of antihypertensive, and use of antihyperglycemic) or from medical records and laboratory measures (e.g., hemoglobin A1c, urine albumin to creatinine ratio) only marginally improved the performance of the models.
The claims-based models developed could reliably predict the risk of cardiovascular events in T2DM patients, without requiring pharmacy claims or laboratory measures. These models could be relevant for providers and payers and help implement approaches to prevent cardiovascular events in high-risk diabetic patients.
存在几种心血管疾病(CVD)预测风险模型,包括一些专门为 2 型糖尿病(T2DM)患者开发的模型。然而,为糖尿病患者开发的模型是基于从病历或实验室结果中获得的信息,这些信息通常无法提供给付款人或医疗质量组织等实体。本研究旨在开发并验证基于医疗保险索赔数据预测 T2DM 患者心血管事件风险的模型。
从 Optum 综合真实世界证据电子健康记录和索赔匿名数据库(2006 年 10 月 1 日至 2016 年 9 月 30 日)中确定年龄在 50 岁或以上的 T2DM 患者。在 12 个月的基线期内评估风险因素,并从基线期结束后监测心血管事件,直至数据可用、连续入组或死亡结束。使用逻辑回归分别为既往有 CVD 和无 CVD 的患者开发风险模型,并为每个结局:(1)主要不良心血管事件(MACE;即非致死性心肌梗死、非致死性卒中和 CVD 相关死亡);(2)任何 MACE、不稳定型心绞痛住院或充血性心力衰竭住院;(3)CVD 相关死亡。分别在样本的 70%和 30%上开发和验证模型。使用 C 统计量评估模型性能。
共确定 181619 例患者,其中 136544 例(75.2%)无既往 CVD,45075 例(24.8%)有 CVD 病史。年龄、糖尿病相关住院治疗、既往 CVD 诊断和慢性肺部疾病是所有模型中最重要的预测因素。C 统计量范围为 0.70 至 0.81,表明模型性能良好。仅略微增加来自药房索赔(如抗高血压药物的使用和抗高血糖药物的使用)或来自病历和实验室测量(如糖化血红蛋白、尿白蛋白与肌酐比)的风险因素并不能显著改善模型性能。
无需药房索赔或实验室测量,基于索赔的模型可可靠预测 T2DM 患者心血管事件的风险。这些模型可能对提供者和付款人有意义,并有助于实施预防高危糖尿病患者心血管事件的方法。