Betsuyaku Tomoko, Kato Motokazu, Fujimoto Keisaku, Kobayashi Akihiro, Hayamizu Tomoyuki, Hitosugi Hideki, Hagan Gerald, James Mark H, Jones Paul W
Division of Pulmonary Medicine, Department of Medicine, Keio University, Tokyo, Japan.
Chest Disease Clinical and Research Institute, Kishiwada City Hospital, Kishiwada, Japan.
Int J Chron Obstruct Pulmon Dis. 2018 Aug 13;13:2409-2423. doi: 10.2147/COPD.S152723. eCollection 2018.
The Global initiative for chronic Obstructive Lung Disease strategy document for COPD recommends treatment changes according to the persistence of symptoms or exacerbations. This study assessed the feasibility and outcomes of a structured step-up/step-down treatment approach in a randomized controlled clinical trial setting.
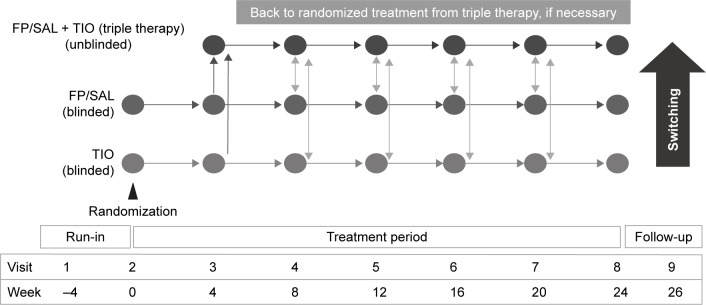
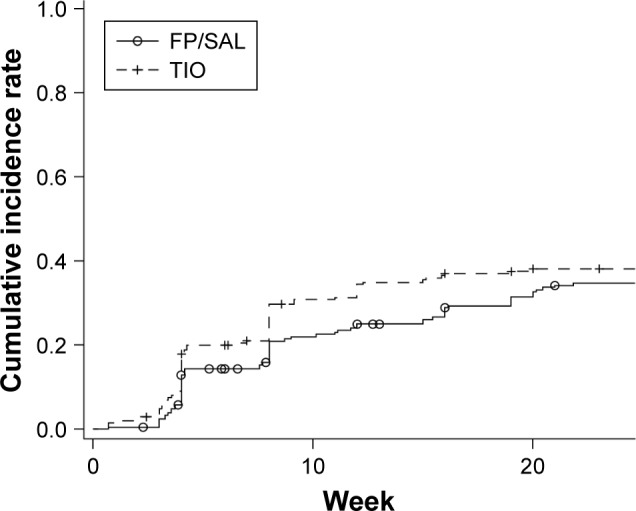
Japanese patients with moderate-to-severe COPD were randomized to blinded, double-dummy treatment with twice-daily fluticasone propionate/salmeterol (FP/SAL) 250/50 µg or once-daily tiotropium bromide (TIO) 18 µg for 24 weeks (dual bronchodilator was not available). At 4-weekly intervals, patients remaining symptomatic (COPD Assessment Test score >10) or experiencing an exacerbation were offered the option to use triple therapy. Primary endpoint was the proportion of patients remaining on randomized therapy.
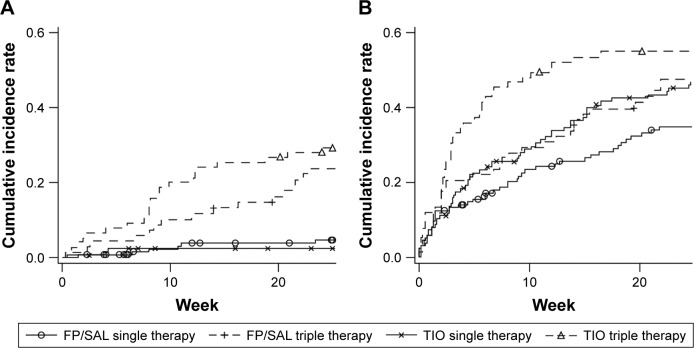
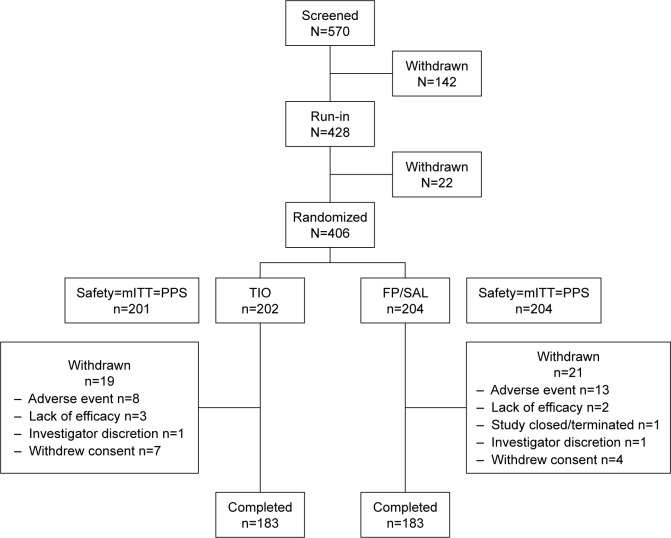
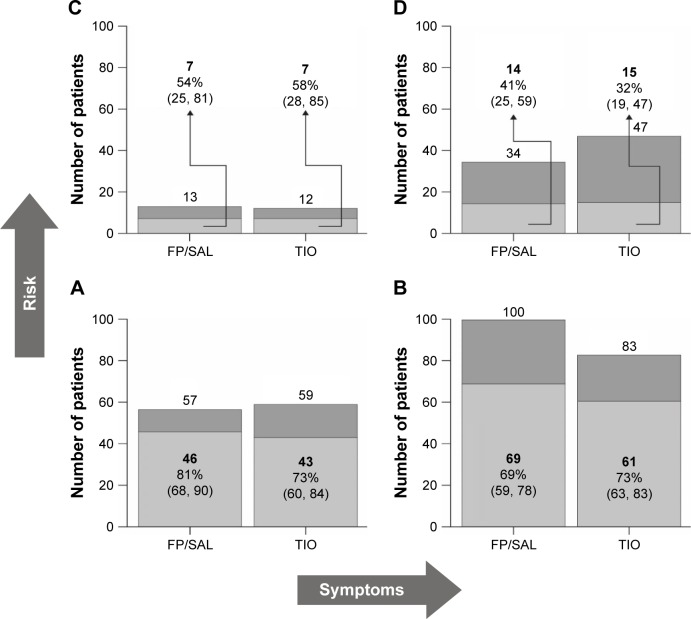
In total, 406 patients participated (mean FEV 59%±13% predicted; COPD Assessment Test 12±6). Of these, 204 and 201 patients were included in the FP/SAL and TIO groups, respectively, of whom 67% and 63% continued treatment throughout the study; this difference was not statistically significant. Time to first therapy switch was longer with FP/SAL, but not significantly (=0.21). More patients in Global initiative for chronic Obstructive Lung Disease (2011 criteria) groups C/D switched (FP/SAL 55%, TIO 63%) than in groups A/B (FP/SAL 27%, TIO 27%).
Given the choice, patients with more symptoms or those experiencing an exacerbation will agree to step-up therapy. Effectiveness of disease management pathways can be tested using double-blind studies.
慢性阻塞性肺疾病全球倡议组织(Global initiative for chronic Obstructive Lung Disease)的慢性阻塞性肺疾病(COPD)策略文件建议根据症状持续或急性加重情况调整治疗方案。本研究在随机对照临床试验环境中评估了结构化的逐步升级/逐步降级治疗方法的可行性和结果。
将日本中重度慢性阻塞性肺疾病患者随机分为两组,分别接受每日两次的丙酸氟替卡松/沙美特罗(FP/SAL)250/50μg或每日一次的噻托溴铵(TIO)18μg的盲法、双模拟治疗,为期24周(当时尚无双重支气管扩张剂)。每隔4周,对仍有症状(慢性阻塞性肺疾病评估测试评分>10)或发生急性加重的患者提供使用三联疗法的选择。主要终点是继续接受随机分组治疗的患者比例。
共有406例患者参与研究(平均第一秒用力呼气容积占预计值的百分比为59%±13%;慢性阻塞性肺疾病评估测试评分为12±6)。其中,分别有204例和201例患者纳入FP/SAL组和TIO组,两组中分别有67%和63%的患者在整个研究期间持续接受治疗;这一差异无统计学意义。FP/SAL组首次治疗转换的时间更长,但差异不显著(P=0.21)。与A/B组(FP/SAL组为27%,TIO组为27%)相比,慢性阻塞性肺疾病全球倡议组织(2011年标准)C/D组中更多患者转换了治疗方案(FP/SAL组为55%,TIO组为63%)。
在有选择的情况下,症状较多或发生急性加重的患者会同意升级治疗。疾病管理途径的有效性可以通过双盲研究进行检验。