Copenhagen Diabetes Foot Center (CODIF), Bispebjerg Hospital, University of Copenhagen, 2400 Copenhagen NV, Denmark.
Department of Endocrinology, Bispebjerg Hospital, University of Copenhagen, 2400 Copenhagen NV, Denmark.
J Diabetes Res. 2018 Aug 2;2018:5647981. doi: 10.1155/2018/5647981. eCollection 2018.
Due to the localized nature of Charcot foot, systemically altered levels of inflammation markers can be difficult to measure. The aim of this study was to investigate whether it is possible to detect an arteriovenous (A-V) flux in any locally produced inflammatory biomarkers from an acute Charcot foot by comparing local and systemic measurements.
We included patients with acute diabetic Charcot foot. Blood was sampled from the vena saphena magna on the distal part of the crus bilaterally as well as from the arteria radialis. To minimize the A-V shunting effect, the feet were externally cooled with ice water prior to resampling.
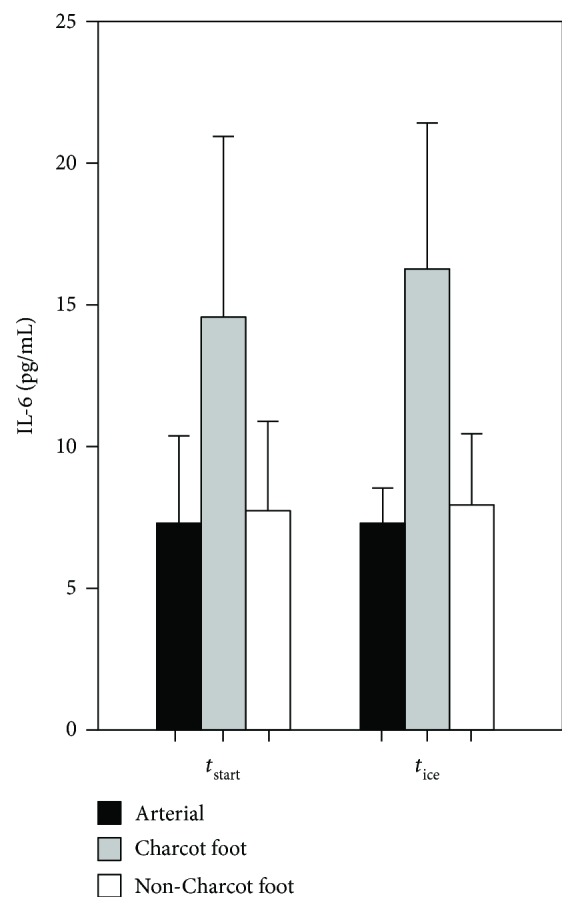
Both before and after cooling, the A-V flux of interleukin-6 (IL-6) between the Charcot feet and the arterial level was significantly higher than the flux between the healthy feet and the arterial level (Δvalue: 7.25 versus 0.41 pg/mL, resp., = 0.008; Δvalue: 10.04 versus 1.68 pg/mL, resp., = 0.032). There were no differences in the fluxes for other markers of inflammation.
We have found an increased A-V flux of IL-6 in the acute diabetic Charcot foot compared to the healthy foot in the same patients.
由于夏科足具有局部性,全身性炎症标志物水平的改变很难测量。本研究旨在通过比较局部和全身测量值,来探讨是否可以从急性夏科足的局部产生的炎症生物标志物中检测到动静脉(A-V)通量。
我们纳入了患有急性糖尿病性夏科足的患者。双侧小腿部大隐静脉及桡动脉均采集血样。为了最小化 A-V 分流效应,在重新取样前,将足部用冰水外部冷却。
在冷却前后,夏科足与动脉水平之间的白细胞介素 6(IL-6)的 A-V 通量均明显高于健康足与动脉水平之间的 A-V 通量(Δ值:7.25 与 0.41 pg/mL, = 0.008;Δ值:10.04 与 1.68 pg/mL, = 0.032)。其他炎症标志物的通量没有差异。
与同一患者的健康足部相比,我们发现急性糖尿病性夏科足的 IL-6 的 A-V 通量增加。