Folestad Agnetha, Ålund Martin, Asteberg Susanne, Fowelin Jesper, Aurell Ylva, Göthlin Jan, Cassuto Jean
Department of Orthopaedics, CapioLundby Hospital, Göteborg, Sweden.
Department of Orthopaedics, Sahlgrenska University Hospital, Mölndal, Sweden.
J Foot Ankle Res. 2015 Dec 10;8:72. doi: 10.1186/s13047-015-0129-y. eCollection 2015.
Proinflammatory cytokines are an integral part of the osteolytic activity of Charcot arthropathy but are also central to normal bone healing. As there are no previous longitudinal studies investigating their role during the recovery phase of Charcot, we set out to monitor systemic levels of proinflammatory cytokines from Charcot presentation until a clinically and radiographically documented chronic state has been reached.
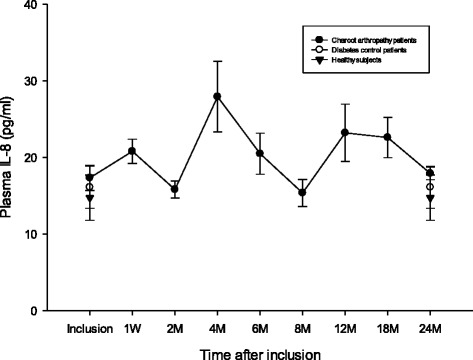
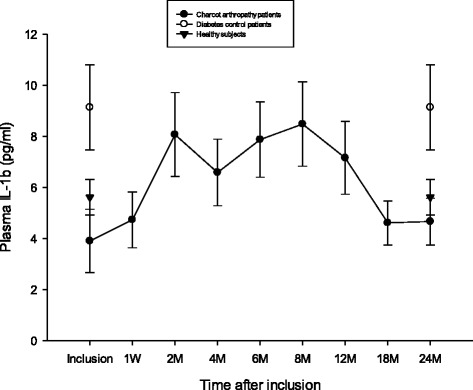
Twenty-eight consecutive Charcot patients were monitored during 2 years by repeated foot radiographs, MRI and plasma levels of interleukin [IL]-6, IL-8, IL-1β, Tumor Necrosis Factor [TNF]-α, and IL-1 receptor antibody (IL-1RA). Charcot patients were treated with total contact cast (TCC) on the first day of inclusion. Neuropathic diabetic controls (n = 20) and Healthy subjects (n = 20) served as reference.
Plasma IL-6, IL-8, IL-1β and TNF-α in the acute and chronic phase of Charcot were below or at the level of diabetic controls and healthy, whereas IL-1RA/IL-1β ratio was continuously higher in Charcot patients. IL-6, TNF-α and IL-1RA began to increase one week after offloading to reach a peak after 4 months before gradually receding.
A sustained increase of IL-6 and TNF-α starting shortly after offloading and paralleled by accelerated bone healing on radiographs, suggest that offloading, by activating the inflammatory stage, has a key role to play in the onset of coupled bone remodeling. High IL-1RA/IL-1β ratio in Charcot patients at presentation supports a counter-balancing anti-inflammatory role for IL-1RA in the acute phase whereas a high ratio after two years, possibly due to renewed weight-bearing on a deformed foot, signal need for continued anti-inflammatory activity and contradicts a "cold" biological state in the chronic phase.
促炎细胞因子是夏科氏关节病溶骨活性的一个组成部分,但也是正常骨愈合的核心。由于此前没有纵向研究调查它们在夏科氏病恢复阶段的作用,我们着手监测从夏科氏病出现到临床和影像学记录的慢性状态达到期间促炎细胞因子的全身水平。
通过重复足部X线片、MRI以及白细胞介素[IL]-6、IL-8、IL-1β、肿瘤坏死因子[TNF]-α和IL-1受体抗体(IL-1RA)的血浆水平,对28例连续的夏科氏病患者进行了2年的监测。夏科氏病患者在纳入的第一天接受全接触石膏(TCC)治疗。神经性糖尿病对照组(n = 20)和健康受试者(n = 20)作为对照。
夏科氏病急性期和慢性期的血浆IL-6、IL-8、IL-1β和TNF-α低于或处于糖尿病对照组和健康组水平,而夏科氏病患者的IL-1RA/IL-1β比值持续较高。卸载后一周,IL-6、TNF-α和IL-1RA开始升高,4个月后达到峰值,然后逐渐下降。
卸载后不久IL-6和TNF-α持续升高,并与X线片上加速的骨愈合同时出现,这表明卸载通过激活炎症阶段,在耦合骨重塑的开始中起关键作用。夏科氏病患者就诊时高IL-1RA/IL-1β比值支持IL-1RA在急性期具有平衡的抗炎作用,而两年后高比值可能由于畸形足部重新负重,表明需要持续的抗炎活性,这与慢性期的“冷”生物学状态相矛盾。