Lofters Aisha K, Mark Amy, Taljaard Monica, Green Michael E, Glazier Richard H, Dahrouge Simone
Department of Family & Community Medicine, St. Michael's Hospital, 30 Bond St, Toronto, ON, M5B1W8, Canada.
Department of Family & Community Medicine, University of Toronto, 500 University Ave. 5th Floor, Toronto, ON, M5G1V7, Canada.
BMC Fam Pract. 2018 Aug 29;19(1):147. doi: 10.1186/s12875-018-0827-1.
Primary care has been reformed in recent years in Ontario, Canada, with a move away from traditional fee-for-service to enhanced fee-for-service and capitation-based models. It is unclear how new models have affected disparities in cancer screening. We evaluated whether Ontario's enhanced fee-for-service model was associated with a change in the gaps in cancer screening for people living with low income and people who are foreign-born.
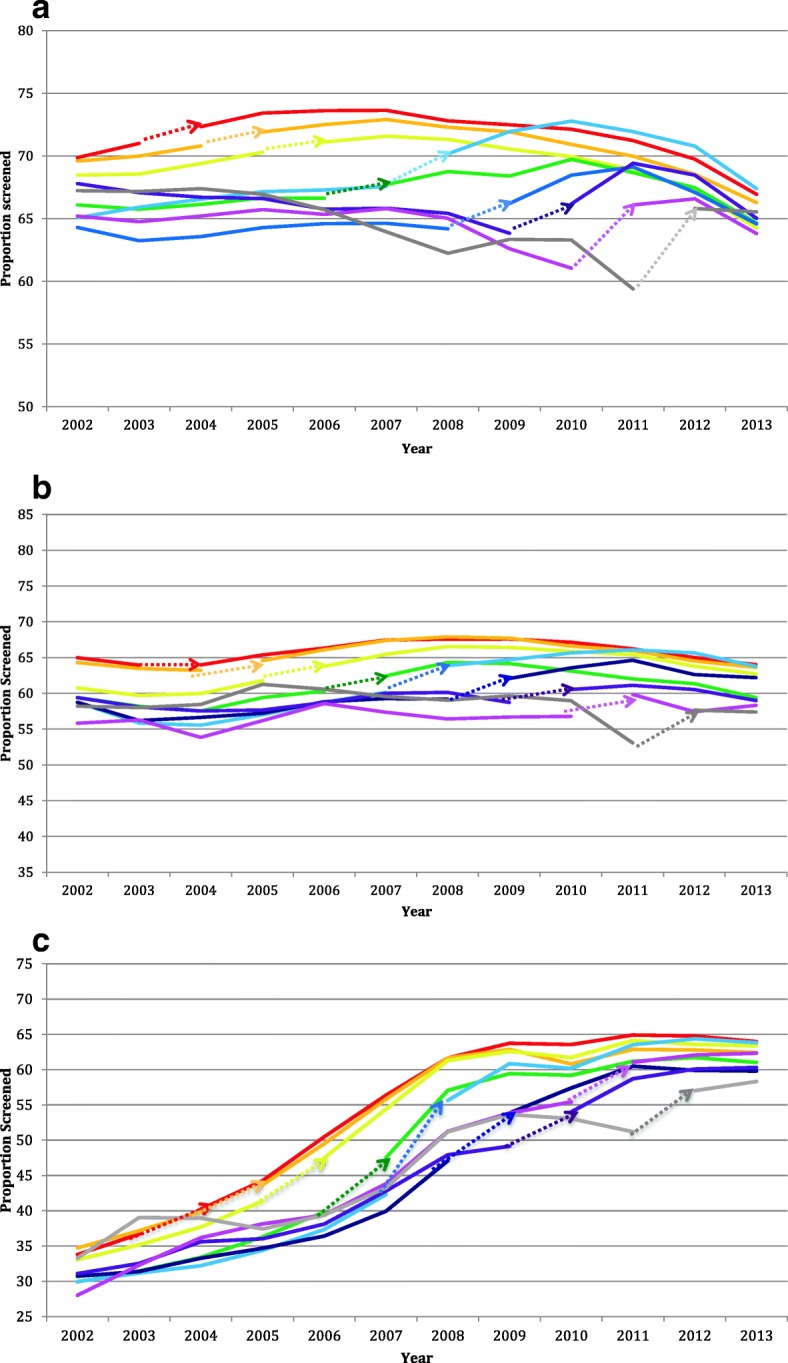
We conducted a population-based longitudinal analysis from 2002 to 2013 of Ontario family physicians who transitioned from traditional fee-for-service to enhanced fee-for-service. The binary outcomes of interest were adherence to cervical, breast and colorectal cancer screening recommendations. Outcomes were analyzed using mixed-effects logistic regression. Analyses produced annual odds ratios comparing the odds of being up-to-date for screening among patients in enhanced fee-for-service versus patients in traditional fee-for-service for each social stratum separately. We calculated the ratios of stratum-specific odds ratios to assess whether the transition from traditional to enhanced fee-for-service was associated with a change in screening gaps between immigrants and long-term residents, and between people in the lowest and highest neighbourhood income quintiles.
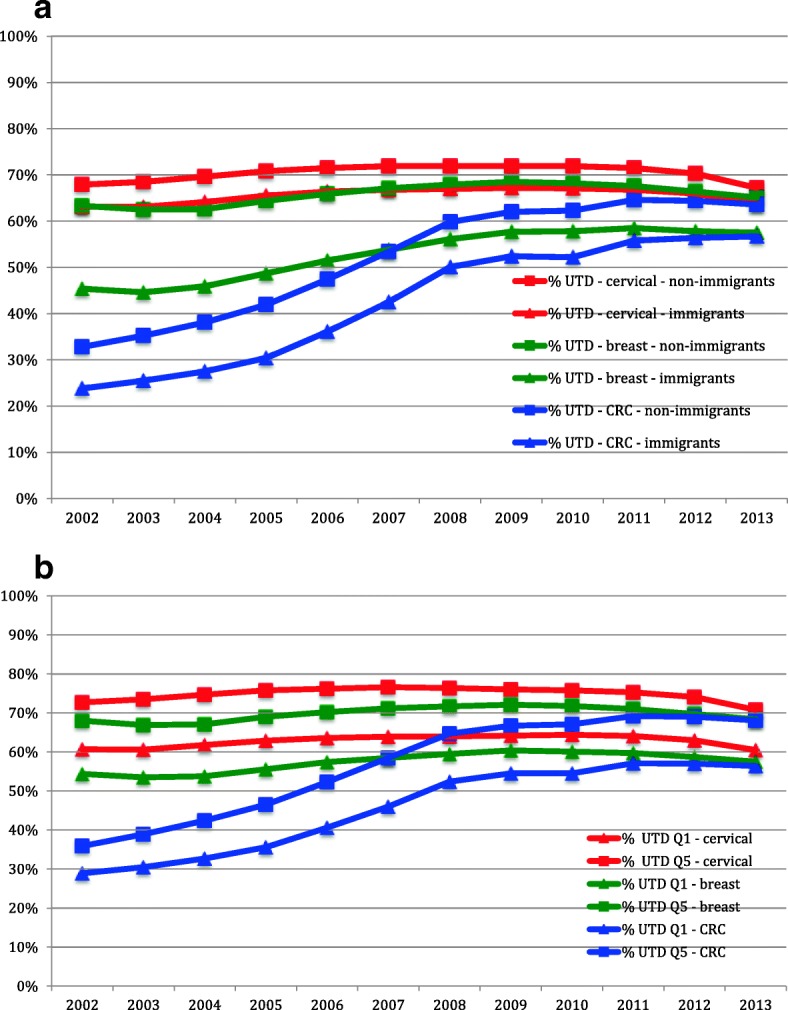
Throughout the study period, cancer screening was consistently lower among immigrants and among people in the lowest income quintile. Transition to enhanced fee-for-service was generally associated with increased screening uptake for all, however for most years, ratios of ratios were significantly less than 1 for all three cancer screening types, indicating that there was a widening of the screening gap between immigrants and long-term residents and between people living in the lowest vs. highest income quintile associated with transitions.
The transition to enhanced fee-for-service in Ontario was generally associated with a widening of screening inequities for foreign-born and low-income patients.
近年来,加拿大安大略省对初级医疗保健进行了改革,从传统的按服务收费模式转向强化按服务收费和基于人头费的模式。目前尚不清楚新模式如何影响癌症筛查方面的差异。我们评估了安大略省的强化按服务收费模式是否与低收入人群和外国出生人群在癌症筛查差距方面的变化有关。
我们对2002年至2013年从传统按服务收费模式转变为强化按服务收费模式的安大略家庭医生进行了基于人群的纵向分析。感兴趣的二元结局是对宫颈癌、乳腺癌和结直肠癌筛查建议的依从性。使用混合效应逻辑回归分析结局。分析分别得出每年的优势比,比较每个社会阶层中强化按服务收费模式下的患者与传统按服务收费模式下的患者进行最新筛查的几率。我们计算了特定阶层优势比的比率,以评估从传统按服务收费模式向强化按服务收费模式的转变是否与移民和长期居民之间以及邻里收入最低和最高五分位数人群之间的筛查差距变化有关。
在整个研究期间,移民和收入最低五分位数人群的癌症筛查率一直较低。向强化按服务收费模式的转变总体上与所有人的筛查接受率增加有关,然而在大多数年份,所有三种癌症筛查类型的比率之比均显著小于1,这表明与转变相关的移民和长期居民之间以及收入最低与最高五分位数人群之间的筛查差距在扩大。
安大略省向强化按服务收费模式的转变总体上与外国出生和低收入患者的筛查不平等加剧有关。