Spitzer Ernest, Ren Ben, Kroon Herbert, van Gils Lennart, Manintveld Olivier, Daemen Joost, Zijlstra Felix, de Jaegere Peter P, Geleijnse Marcel L, Van Mieghem Nicolas M
Department of Cardiology, Thoraxcenter, Erasmus University Medical Center, Rotterdam, Netherlands.
Cardialysis, Clinical Trial Management and Core Laboratories, Rotterdam, Netherlands.
Front Cardiovasc Med. 2018 Aug 17;5:111. doi: 10.3389/fcvm.2018.00111. eCollection 2018.
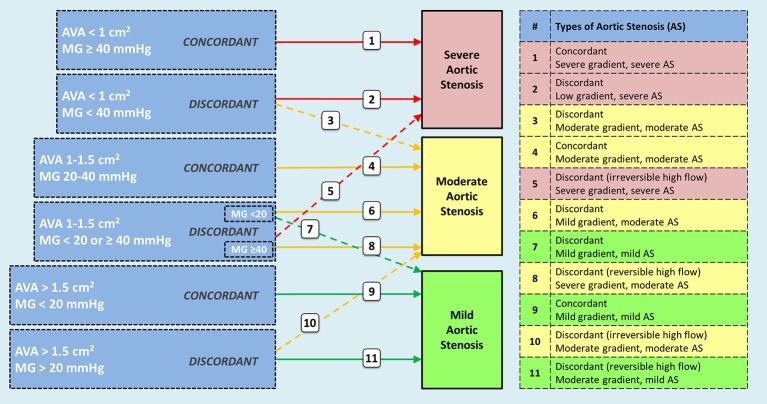
Moderate aortic stenosis (AS) and reduced left ventricular ejection fraction (LVEF) constitute a clinical entity that has been proposed as a therapeutic target for transcatheter aortic valve replacement (TAVR). It is defined by a mean trans-aortic gradient between 20 and 40 mmHg and an aortic valve area between 1.0 and 1.5 cm in patients with LVEF < 50%. Retrospective data suggests a prevalence of 0.8% among patients referred for echocardiographic assessment. These patients are younger and show a higher frequency of previous myocardial infarction than those with severe AS randomized to TAVR in recent trials. In two retrospective studies including patients with moderate AS and reduced LVEF, a one-year mortality rate of 9 and 32% was reported, the latter in patients treated with medical therapy only during follow-up. Echocardiographic diagnosis of moderate AS poses challenges as current guidelines are directed to determine severe AS, and different presentations of moderate and mild AS have been generally neglected. Thus, the nomenclature would need to be revised and a description of possible scenarios is provided in this review. Dobutamine stress echocardiography and computed tomography are promising complementary tools. Likewise, a standardized clinical pathway is needed, in which a high level of suspicion and a low threshold for referral to a heart valve center is warranted. The Transcatheter Aortic Valve Replacement to UNload the Left ventricle in patients with Advanced heart failure (TAVR UNLOAD) trial (NCT02661451) is exploring whether TAVR would improve outcomes in patients receiving optimal heart failure therapy.
中度主动脉瓣狭窄(AS)和左心室射血分数(LVEF)降低构成了一种临床实体,已被提议作为经导管主动脉瓣置换术(TAVR)的治疗靶点。其定义为LVEF<50%的患者,平均跨主动脉压差在20至40 mmHg之间,主动脉瓣面积在1.0至1.5平方厘米之间。回顾性数据表明,在接受超声心动图评估的患者中,其患病率为0.8%。与近期试验中随机接受TAVR治疗的重度AS患者相比,这些患者更年轻,既往心肌梗死的发生率更高。在两项纳入中度AS和LVEF降低患者的回顾性研究中,报告的一年死亡率分别为9%和32%,后者是仅在随访期间接受药物治疗的患者。中度AS的超声心动图诊断存在挑战,因为当前指南旨在确定重度AS,而中度和轻度AS的不同表现通常被忽视。因此,需要修订命名法,本综述提供了可能情况的描述。多巴酚丁胺负荷超声心动图和计算机断层扫描是有前景的辅助工具。同样,需要一个标准化的临床路径,其中需要高度怀疑并降低转诊至心脏瓣膜中心的阈值。晚期心力衰竭患者经导管主动脉瓣置换术减轻左心室负荷(TAVR UNLOAD)试验(NCT02661451)正在探索TAVR是否能改善接受最佳心力衰竭治疗患者的预后。