Department of Health Services and Population Research,King's College London, Institute of Psychiatry, Psychology & Neuroscience,London,UK.
Department of Psychological Medicine,King's College London, Institute of Psychiatry, Psychology & Neuroscience,London,UK.
Psychol Med. 2019 Jul;49(10):1639-1651. doi: 10.1017/S0033291718002210. Epub 2018 Sep 5.
Depression is associated with increased mortality, however, little is known about its variation by ethnicity.
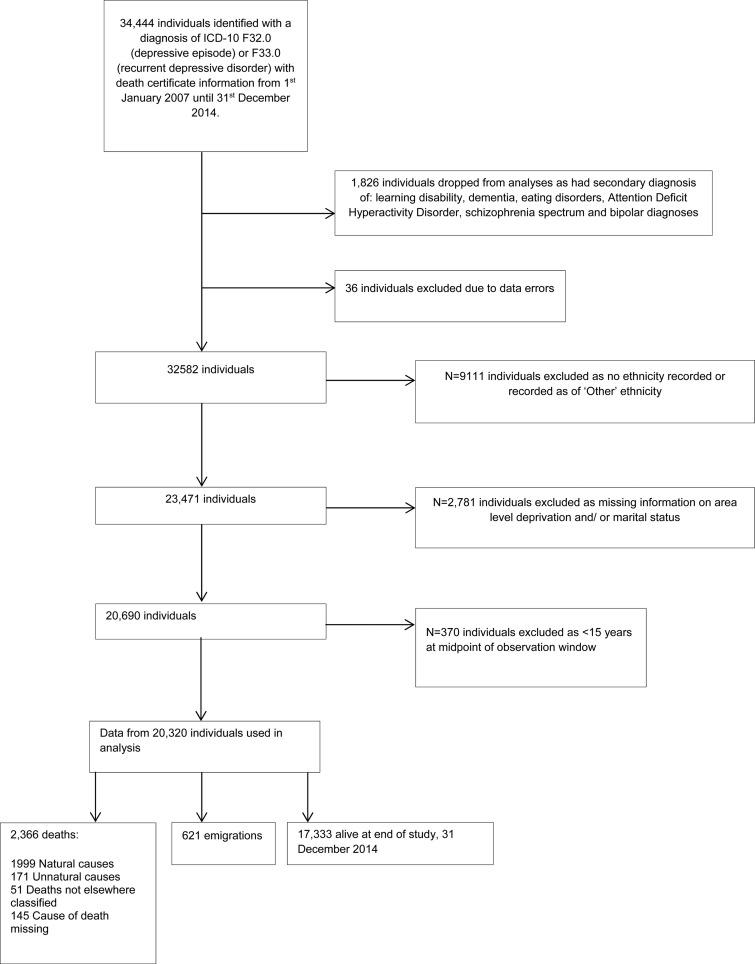
We conducted a cohort study of individuals with ICD-10 unipolar depression from secondary mental healthcare, from an ethnically diverse location in southeast London, followed for 8 years (2007-2014) linked to death certificates. Age- and sex- standardised mortality ratios (SMRs), with the population of England and Wales as a standard population were derived. Hazard ratios (HRs) for mortality were derived through multivariable regression procedures.
Data from 20 320 individuals contributing 91 635 person-years at risk with 2366 deaths were used for analyses. SMR for all-cause mortality in depression was 2.55(95% CI 2.45-2.65), with similar trends by ethnicity. Within the cohort with unipolar depression, adjusted HR (aHRs) for all-cause mortality in ethnic minority groups relative to the White British group were 0.62(95% CI 0.53-0.74) (Black Caribbean), 0.53(95% CI 0.39-0.72) (Black African) and 0.69(95% CI 0.52-0.90) (South Asian). Male sex and alcohol/substance misuse were associated with an increased all-cause mortality risk [aHR:1.94 (95% CI 1.68-2.24) and aHR:1.18 (95% CI 1.01-1.37) respectively], whereas comorbid anxiety was associated with a decreased risk [aHR: 0.72(95% CI 0.58-0.89)]. Similar associations were noted for natural-cause mortality. Alcohol/substance misuse and male sex were associated with a near-doubling in unnatural-cause mortality risk, whereas Black Caribbean individuals with depression had a reduced unnatural-cause mortality risk, relative to White British people with depression.
Although individuals with depression experience an increased mortality risk, marked heterogeneity exists by ethnicity. Research and practice should focus on addressing tractable causes underlying increased mortality in depression.
抑郁症与死亡率增加有关,但关于其在不同种族之间的差异知之甚少。
我们进行了一项队列研究,纳入了来自伦敦东南部一个种族多样化地区二级精神保健机构的 ICD-10 单相抑郁症患者,随访 8 年(2007-2014 年),并与死亡证明相关联。采用年龄和性别标准化死亡率比(SMR),以英格兰和威尔士的人口为标准人群。通过多变量回归程序得出死亡率的危险比(HR)。
我们使用了 20320 名患者的数据,这些患者共贡献了 91635 人年的风险,有 2366 人死亡。抑郁症患者的全因死亡率的 SMR 为 2.55(95%CI 2.45-2.65),不同种族之间的趋势相似。在单相抑郁症患者队列中,与白种英国人相比,少数民族群体的全因死亡率的调整 HR(aHR)分别为 0.62(95%CI 0.53-0.74)(加勒比黑人)、0.53(95%CI 0.39-0.72)(非洲黑人)和 0.69(95%CI 0.52-0.90)(南亚人)。男性和酒精/物质滥用与全因死亡率风险增加相关[aHR:1.94(95%CI 1.68-2.24)和 aHR:1.18(95%CI 1.01-1.37)],而共病焦虑与风险降低相关[aHR:0.72(95%CI 0.58-0.89)]。自然原因死亡率也有类似的关联。酒精/物质滥用和男性与非自然原因死亡率风险增加近一倍有关,而与白种英国人相比,患有抑郁症的加勒比黑人的非自然原因死亡率风险降低。
尽管抑郁症患者的死亡率增加,但不同种族之间存在显著的异质性。研究和实践应集中于解决导致抑郁症死亡率增加的可处理原因。