Bareham Corinne A, Allanson Judith, Roberts Neil, Hutchinson Peter J A, Pickard John D, Menon David K, Chennu Srivas
Department of Clinical Neurosciences, University of Cambridge, Cambridge, United Kingdom.
Cambridge University Hospitals NHS Foundation Trust, Cambridge, United Kingdom.
Front Neurol. 2018 Aug 21;9:676. doi: 10.3389/fneur.2018.00676. eCollection 2018.
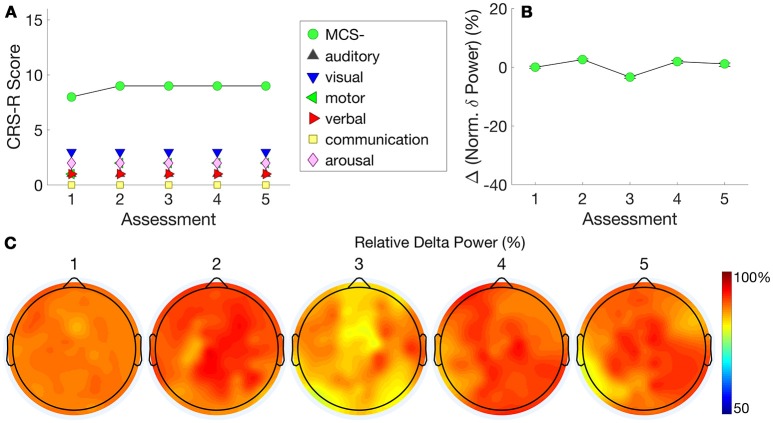
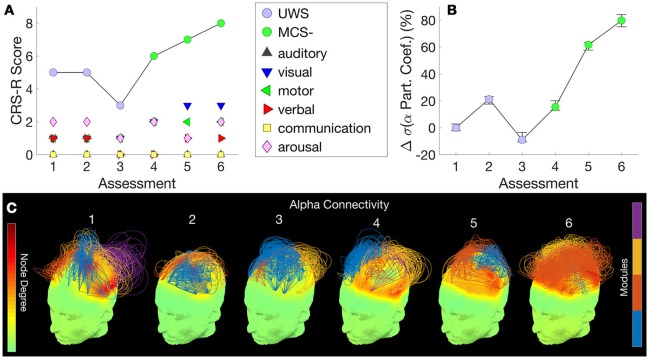
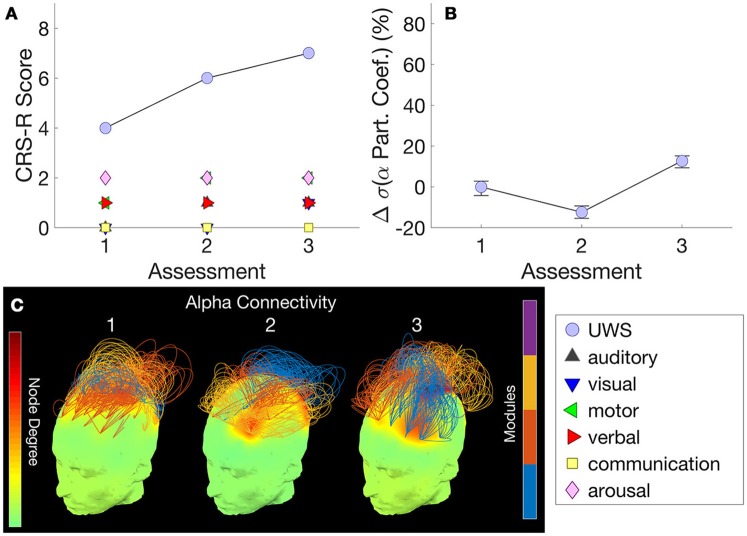
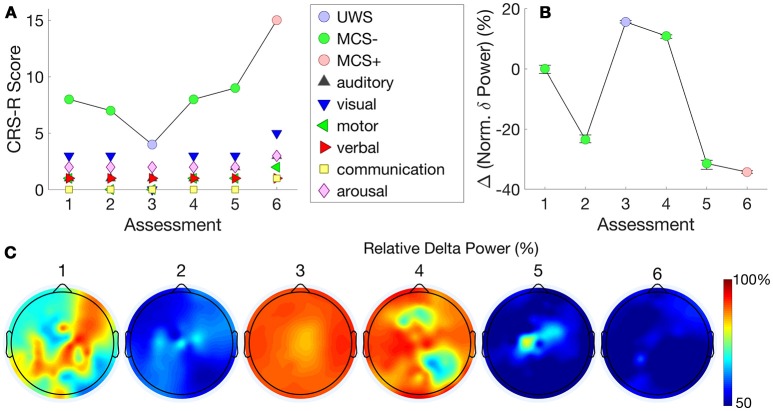
Clinicians are regularly faced with the difficult challenge of diagnosing consciousness after severe brain injury. As such, as many as 40% of minimally conscious patients who demonstrate fluctuations in arousal and awareness are known to be misdiagnosed as unresponsive/vegetative based on clinical consensus. Further, a significant minority of patients show evidence of hidden awareness not evident in their behavior. Despite this, clinical assessments of behavior are commonly used as bedside indicators of consciousness. Recent advances in functional high-density electroencephalography (hdEEG) have indicated that specific patterns of resting brain connectivity measured at the bedside are strongly correlated with the re-emergence of consciousness after brain injury. We report case studies of four patients with traumatic brain injury who underwent regular assessments of hdEEG connectivity and Coma Recovery Scale-Revised (CRS-R) at the bedside, as part of an ongoing longitudinal study. The first, a patient in an unresponsive wakefulness state (UWS), progressed to a minimally-conscious state several years after injury. HdEEG measures of alpha network centrality in this patient tracked this behavioral improvement. The second patient, contrasted with patient 1, presented with a persistent UWS diagnosis that paralleled with stability on the same alpha network centrality measure. Patient 3, diagnosed as minimally conscious minus (MCS-), demonstrated a significant late increase in behavioral awareness to minimally conscious plus (MCS+). This patient's hdEEG connectivity across the previous 18 months showed a trajectory consistent with this increase alongside a decrease in delta power. Patient 4 contrasted with patient 3, with a persistent MCS- diagnosis that was similarly tracked by consistently high delta power over time. Across these contrasting cases, hdEEG connectivity captures both stability and recovery of behavioral trajectories both within and between patients. Our preliminary findings highlight the feasibility of bedside hdEEG assessments in the rehabilitation context and suggest that they can complement clinical evaluation with portable, accurate and timely generation of brain-based patient profiles. Further, such hdEEG assessments could be used to estimate the potential utility of complementary neuroimaging assessments, and to evaluate the efficacy of interventions.
临床医生经常面临诊断严重脑损伤后意识状态的艰巨挑战。因此,据临床共识所知,多达40%表现出觉醒和意识波动的最低意识状态患者被误诊为无反应/植物人状态。此外,少数患者表现出行为中不明显的隐藏意识迹象。尽管如此,行为的临床评估通常被用作意识的床边指标。功能性高密度脑电图(hdEEG)的最新进展表明,在床边测量的静息脑连接的特定模式与脑损伤后意识的重新出现密切相关。作为一项正在进行的纵向研究的一部分,我们报告了4例创伤性脑损伤患者的病例研究,这些患者在床边接受了hdEEG连接性和昏迷恢复量表修订版(CRS-R)的定期评估。第一例是一名处于无反应觉醒状态(UWS)的患者,受伤几年后进展为最低意识状态。该患者阿尔法网络中心性的hdEEG测量结果跟踪了这种行为改善。第二例患者与第一例患者形成对比,持续被诊断为UWS,同时在相同的阿尔法网络中心性测量中保持稳定。第三例患者被诊断为最低意识减(MCS-),后期行为意识显著提高至最低意识加(MCS+)。该患者在过去18个月中的hdEEG连接性显示出与这种增加一致的轨迹,同时δ波功率降低。第四例患者与第三例患者形成对比,持续被诊断为MCS-,随着时间的推移,其δ波功率持续较高,同样被跟踪到。在这些对比病例中,hdEEG连接性捕捉了患者内部和患者之间行为轨迹的稳定性和恢复情况。我们的初步研究结果突出了在康复环境中进行床边hdEEG评估的可行性,并表明它们可以通过便携、准确和及时生成基于大脑的患者概况来补充临床评估。此外,这种hdEEG评估可用于估计补充神经影像学评估的潜在效用,并评估干预措施的疗效。