Tedesco Dario, Gibertoni Dino, Rucci Paola, Hernandez-Boussard Tina, Rosa Simona, Bianciardi Luca, Rolli Maurizia, Fantini Maria Pia
Department of Biomedical and Neuromotor Sciences, University of Bologna, Via San Giacomo, 12, 40126, Bologna, Italy.
Department of Medicine, Stanford University, 1265 Welch Road, 94305, Stanford, California, USA.
BMC Health Serv Res. 2018 Sep 10;18(1):701. doi: 10.1186/s12913-018-3523-x.
Hip fracture in elderly patients is a rising global public health concern because of population ageing, and increasing frailty. Long-term morbidity related to poor management of hip fracture is associated with decreased quality of life, survival, and increase in healthcare costs. Receiving postoperative rehabilitation is associated with better outcomes and a higher likelihood of returning to pre-existing level of functioning. However little is known about which postoperative rehabilitation pathways are more effective to optimize patient outcomes. Few studies have analyzed postoperative rehabilitation pathways in a universal healthcare system. The aim of this study is to analyze the impact of post-acute rehabilitation pathways on mortality and readmission in elderly patients undergoing surgery for hip fracture in a large metropolitan area in Italy.
In this retrospective cohort study, we analyzed 6-month mortality from admission and 6-month readmission after hospital discharge in patients who underwent surgical repair for hip fracture in the hospitals of the Bologna metropolitan area between 1.1.2013 and 30.6.2014. Data were drawn from the regional hospital discharge records database. Kaplan-Meier estimates and multiple Cox regression were used to analyze mortality as a function of rehabilitation pathways. Multiple logistic regression determined predictors of readmission.
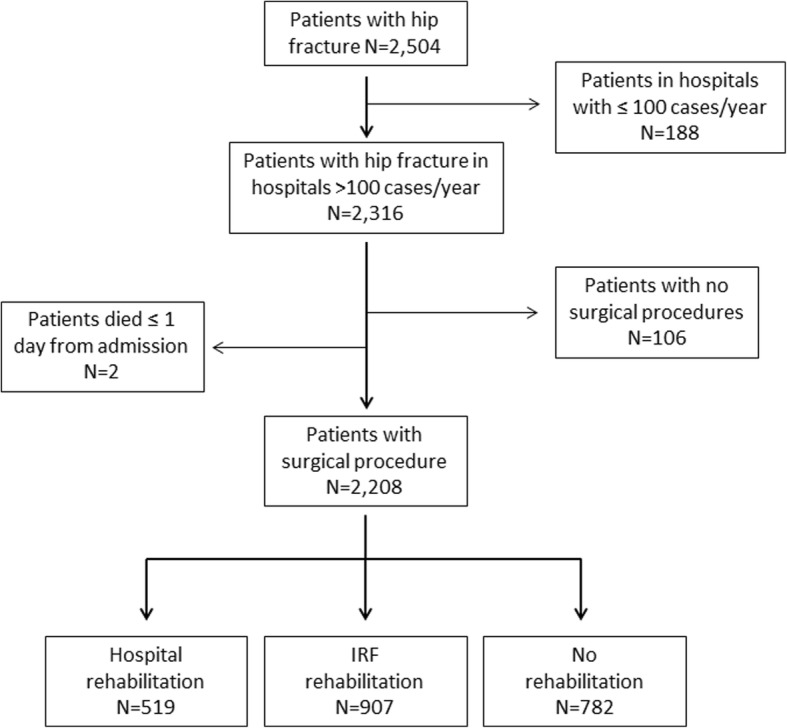
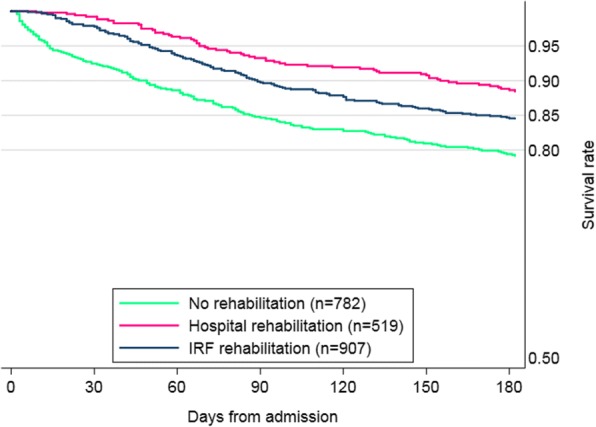
The study population includes 2208 patients, mostly women (n = 1677, 76%), with a median age of 83.8 years. Hospital rehabilitation was provided to 519 patients (23.5%), 907 (41.1%) received rehabilitation in private inpatient rehabilitation facilities (IRF) accredited by the National Health System, and 782 (35.4%) received no post-acute rehabilitation. Compared with patient receiving hospital rehabilitation, the other groups showed significantly higher mortality risks (no rehabilitation, Hazard Ratio (HR) = 2.19, 95%CI = 1.54-3.12, p < 0.001; IRF rehabilitation, HR = 1.66, 95%CI = 1.54-1.79, p < 0.001). The risk of readmission did not differ significantly among rehabilitation pathways.
Intensive hospital rehabilitation was significantly associated with a lower risk of mortality compared to IRF rehabilitation and no rehabilitation. Our results may help in the development of evidence-based recommendations aimed to improve resource utilization and quality of care in hip fracture patients. Further research is warranted to investigate the impact of the rehabilitation pathway on other outcomes, such as patients' functional status and quality of life.
由于人口老龄化以及身体机能衰退,老年患者髋部骨折已成为一个日益严重的全球公共卫生问题。与髋部骨折管理不善相关的长期发病率与生活质量下降、生存率降低以及医疗成本增加有关。接受术后康复治疗与更好的治疗效果以及恢复到先前功能水平的更高可能性相关。然而,对于哪种术后康复途径能更有效地优化患者治疗效果,人们知之甚少。很少有研究在全民医疗体系中分析术后康复途径。本研究的目的是分析急性后期康复途径对意大利一个大都市地区接受髋部骨折手术的老年患者死亡率和再入院率的影响。
在这项回顾性队列研究中,我们分析了2013年1月1日至2014年6月30日期间在博洛尼亚大都市地区医院接受髋部骨折手术修复的患者入院后6个月的死亡率和出院后6个月的再入院率。数据来自地区医院出院记录数据库。采用Kaplan-Meier估计法和多因素Cox回归分析死亡率与康复途径的关系。多因素logistic回归确定再入院的预测因素。
研究人群包括2208例患者,大多数为女性(n = 1677,76%),中位年龄为83.8岁。519例患者(23.5%)接受了医院康复治疗,907例(41.1%)在国家卫生系统认可的私立住院康复机构(IRF)接受康复治疗,782例(35.4%)未接受急性后期康复治疗。与接受医院康复治疗的患者相比,其他组的死亡风险显著更高(未康复,风险比(HR)= 2.19,95%置信区间(CI)= 1.54 - 3.12,p < 0.001;IRF康复,HR = 1.66,95%CI = 1.54 - 1.79,p < 0.001)。不同康复途径之间的再入院风险没有显著差异。
与IRF康复治疗和未康复相比,强化医院康复治疗与较低的死亡风险显著相关。我们的研究结果可能有助于制定基于证据的建议,以提高髋部骨折患者的资源利用和护理质量。有必要进一步研究康复途径对其他结局的影响,如患者的功能状态和生活质量。