Huntington Susie E, Burns Richéal M, Harding-Esch Emma, Harvey Michael J, Hill-Tout Rachel, Fuller Sebastian S, Adams Elisabeth J, Sadiq S Tariq
Aquarius Population Health, 58a Highgate High Street, London, UK.
Health Economics and Policy Analysis Centre (HEPAC), NUI Galway, Ireland.
BMJ Open. 2018 Sep 10;8(9):e020394. doi: 10.1136/bmjopen-2017-020394.
To quantify the costs, benefits and cost-effectiveness of three multipathogen point-of-care (POC) testing strategies for detecting common sexually transmitted infections (STIs) compared with standard laboratory testing.
Modelling study.
Genitourinary medicine (GUM) services in England.
A hypothetical cohort of 965 988 people, representing the annual number attending GUM services symptomatic of lower genitourinary tract infection.
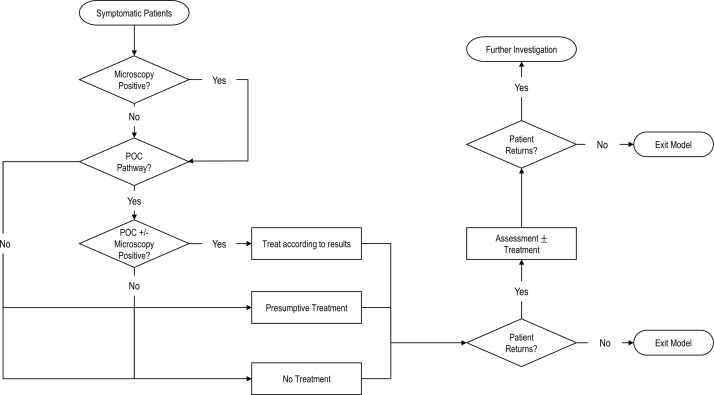
The decision tree model considered costs and reimbursement to GUM services associated with diagnosing and managing STIs. Three strategies using hypothetical point-of-care tests (POCTs) were compared with standard care (SC) using laboratory-based testing. The strategies were: A) dual POCT for (CT) and (NG); B) triplex POCT for CT-NG and (MG); C) quadruplex POCT for CT-NG-MG and (TV). Data came from published literature and unpublished estimates.
Primary outcomes were total costs and benefits (quality-adjusted life years (QALYs)) for each strategy (2016 GB, £) and associated incremental cost-effectiveness ratios (ICERs) between each of the POC strategies and SC. Secondary outcomes were inappropriate treatment of STIs, onward STI transmission, pelvic inflammatory disease in women, time to cure and total attendances.
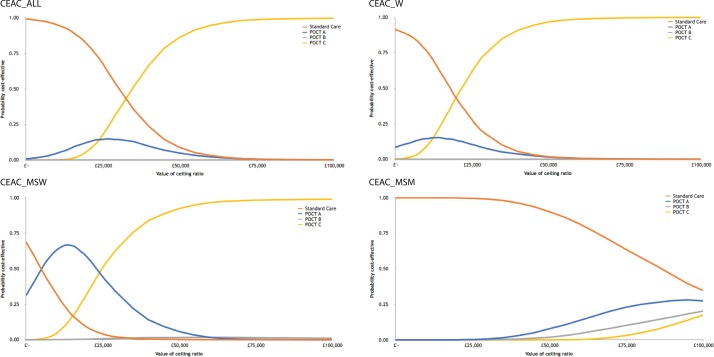
In the base-case analysis, POC strategy C, a quadruplex POCT, was the most cost-effective relative to the other strategies, with an ICER of £36 585 per QALY gained compared with SC when using microcosting, and cost-savings of £26 451 382 when using tariff costing. POC strategy C also generated the most benefits, with 240 467 fewer clinic attendances, 808 fewer onward STI transmissions and 235 135 averted inappropriate treatments compared with SC.
Many benefits can be achieved by using multipathogen POCTs to improve STI diagnosis and management. Further evidence is needed on the underlying prevalence of STIs and SC delivery in the UK to reduce uncertainty in economic analyses.
与标准实验室检测相比,对三种用于检测常见性传播感染(STIs)的多病原体即时检测(POC)策略的成本、效益和成本效益进行量化。
建模研究。
英国的性健康诊所(GUM)服务。
一个假设队列,共965988人,代表每年因下生殖道感染症状就诊于性健康诊所的人数。
决策树模型考虑了与性传播感染诊断和管理相关的性健康诊所服务的成本和报销情况。将三种使用假设即时检测(POCT)的策略与使用基于实验室检测的标准护理(SC)进行比较。这些策略分别是:A)针对沙眼衣原体(CT)和淋病奈瑟菌(NG)的双联POCT;B)针对CT - NG和生殖支原体(MG)的三联POCT;C)针对CT - NG - MG和阴道毛滴虫(TV)的四联POCT。数据来自已发表的文献和未发表的估计。
主要结局是每种策略的总成本和效益(质量调整生命年(QALYs))(2016年英国英镑)以及每种即时检测策略与标准护理之间相关的增量成本效益比(ICERs)。次要结局是性传播感染的不适当治疗、性传播感染的后续传播、女性盆腔炎、治愈时间和总就诊次数。
在基础病例分析中,即时检测策略C(四联POCT)相对于其他策略最具成本效益,使用微观成本核算时,与标准护理相比,每获得一个QALY的ICER为36585英镑,使用费率成本核算时节省成本26451382英镑。与标准护理相比,即时检测策略C还产生了最大的效益,诊所就诊次数减少240467次,性传播感染后续传播减少808次,避免不适当治疗235135例。
使用多病原体POCT改善性传播感染的诊断和管理可带来诸多益处。需要进一步了解英国性传播感染的潜在流行率和标准护理的实施情况,以减少经济分析中的不确定性。