Department of Cardiology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea.
Department of Internal Medicine, Seoul National University Hospital, Seoul, Korea.
Heart. 2020 Jan;106(1):50-57. doi: 10.1136/heartjnl-2018-313242. Epub 2018 Sep 12.
Myocardial ischaemia is a leading cause of acute heart failure (AHF). However, optimal revascularisation strategies in AHF are unclear. We aimed to compare two revascularisation strategies, coronary artery bypass graft (CABG) and percutaneous coronary intervention (PCI), in patients with AHF.
Among 5625 consecutive patients enrolled prospectively in the Korean Acute Heart Failure registry from March 2011 to February 2014, 717 patients who received CABG or PCI during the index hospitalisation for AHF were included in this analysis. We compared adverse outcomes (death, rehospitalisation for HF aggravation or cardiovascular causes, ischaemic stroke and a composite outcome of death and rehospitalisation for HF aggravation or cardiovascular causes) with the use of propensity score matching.
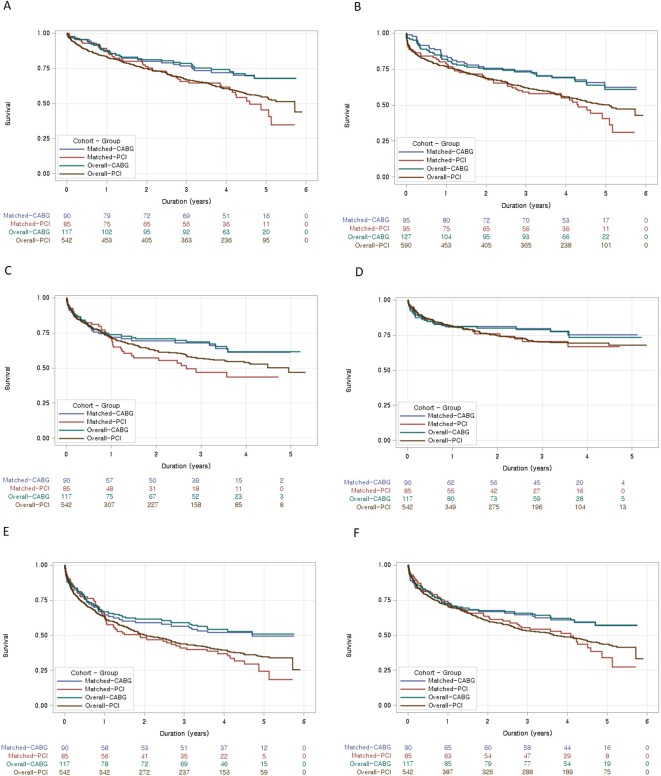
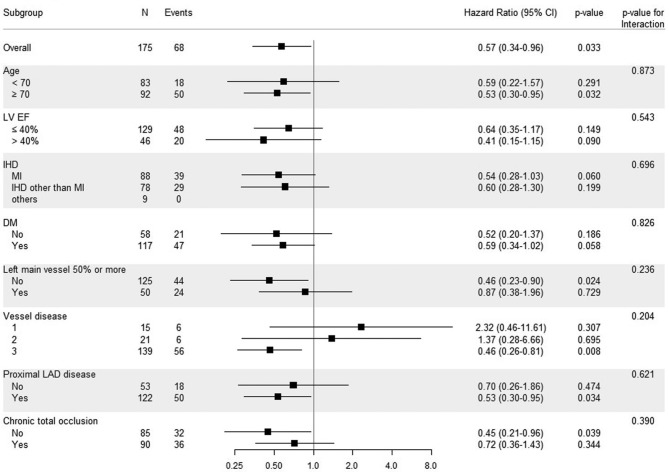
For the propensity score-matched cohort with 190 patients, CABG had a lower risk of all-cause mortality than PCI (83 vs 147 deaths per 1000 patient-years; HR 0.57, 95% CI 0.34 to 0.96, p=0.033) during the median follow-up of 4 years. There was also a trend towards lower rates of rehospitalisation due to cardiovascular events or HF aggravation. Subgroup analysis revealed that the adverse outcomes were significantly lower in the CABG group than in PCI group, especially in patients with old age, three-vessel diseases, significant proximal left anterior descending artery disease and those without left main vessel disease or chronic total occlusion.
Compared with PCI, CABG is associated with significant lower all-cause mortality in patients with AHF. Further studies should evaluate proper revascularisation strategies in AHF.
NCT01389843; Results.
心肌缺血是急性心力衰竭(AHF)的主要原因。然而,AHF 的最佳血运重建策略仍不明确。我们旨在比较两种血运重建策略,即冠状动脉旁路移植术(CABG)和经皮冠状动脉介入治疗(PCI),在 AHF 患者中的应用。
在 2011 年 3 月至 2014 年 2 月期间前瞻性纳入的韩国急性心力衰竭注册研究的 5625 例连续患者中,有 717 例患者在 AHF 指数住院期间接受了 CABG 或 PCI,本分析纳入了这部分患者。我们比较了使用倾向评分匹配后的不良结局(死亡、因 HF 加重或心血管原因再住院、缺血性卒中和死亡和因 HF 加重或心血管原因再住院的复合结局)。
在 190 例倾向评分匹配患者的队列中,在中位随访 4 年期间,CABG 的全因死亡率低于 PCI(每 1000 例患者年分别为 83 例和 147 例死亡;HR 0.57,95%CI 0.34 至 0.96,p=0.033)。因心血管事件或 HF 加重而再住院的发生率也呈下降趋势。亚组分析显示,CABG 组的不良结局明显低于 PCI 组,尤其是在老年、三血管疾病、左前降支近端显著病变和无左主干病变或慢性完全闭塞的患者中。
与 PCI 相比,CABG 与 AHF 患者的全因死亡率显著降低相关。需要进一步的研究来评估 AHF 患者的适当血运重建策略。
NCT01389843;结果。