Lee Chuy Katherine, Velazquez Eric J, Lansky Alexandra J, Jamil Yasser, Ahmad Yousif
Division of Cardiology, Loma Linda University Medical Center, Loma Linda, California.
Section of Cardiovascular Medicine, Yale School of Medicine, New Haven, Connecticut.
J Soc Cardiovasc Angiogr Interv. 2023 Dec 4;2(6Part B):101197. doi: 10.1016/j.jscai.2023.101197. eCollection 2023 Nov-Dec.
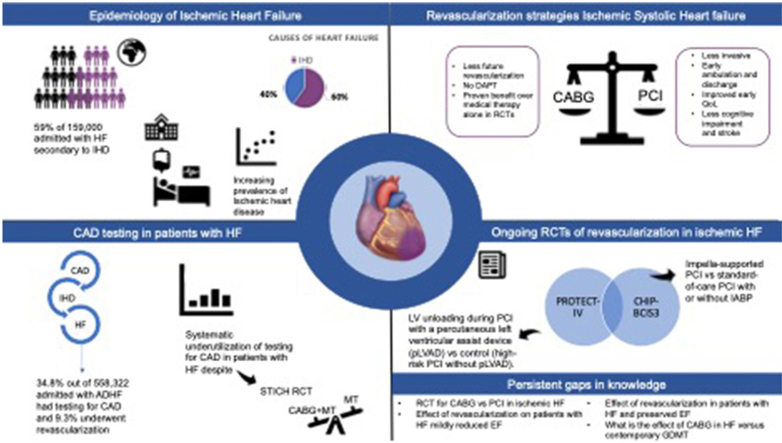
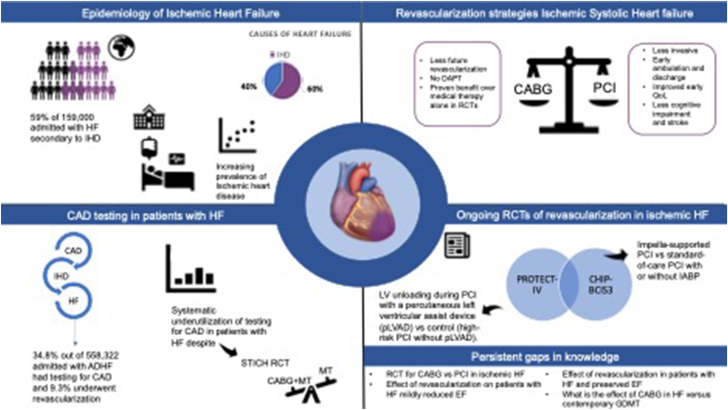
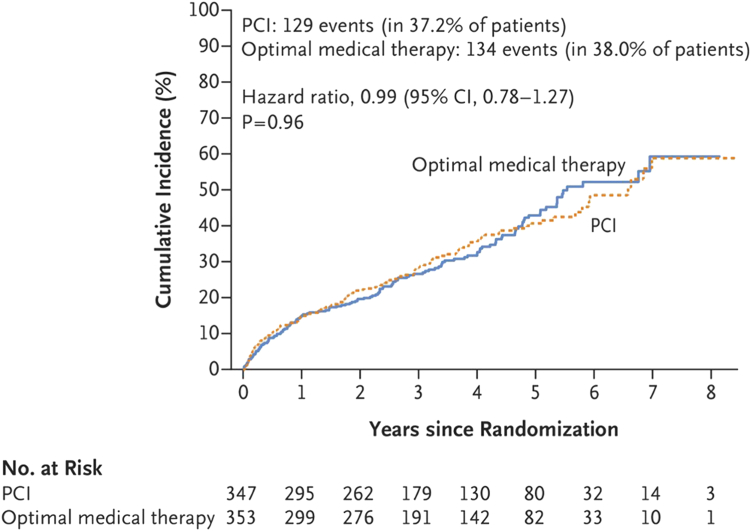
Ischemic heart disease is the largest cause of death worldwide and the most common cause of heart failure (HF). The incidence and prevalence of HF are increasing owing to an aging population and improvements in the acute cardiac care of previously fatal conditions such as myocardial infarction. Strategies to improve outcomes in patients with ischemic systolic HF are urgently needed. There is systematic underutilization of testing for coronary artery disease in patients with HF, and revascularization is performed in an even smaller minority despite evidence for reduced mortality with coronary artery bypass grafting (CABG) over medical therapy in the Surgical Treatment for Ischemic Heart Failure Extension Study. Percutaneous coronary intervention (PCI) is a less-invasive approach to coronary revascularization; however, the recent Revascularization for Ischemic Ventricular Dysfunction (REVIVED)-British Cardiovascular Intervention Society (BCIS2) trial failed to demonstrate a benefit of PCI compared with that of medical therapy in patients with ischemic systolic HF. The comparative effectiveness of PCI and CABG for patients with ischemic systolic HF remains unknown, particularly in the era of contemporary medical therapy. In this review, we discuss the benefit of CABG in ischemic systolic HF, its underutilization, and the unmet clinical need. We also review the recent REVIVED-BCIS2 trial comparing PCI to medical therapy, as well as upcoming randomized controlled trials of PCI for ischemic systolic HF and persistent evidence gaps that will exist despite anticipated data from ongoing trials. There remains a need for an adequately powered randomized controlled trials to establish the comparative clinical effectiveness of PCI vs CABG in ischemic systolic HF in the era of contemporary revascularization approaches and medical therapy, as well as trials of coronary revascularization in patients with HF with preserved ejection fraction or less severe forms of left ventricular systolic dysfunction.
缺血性心脏病是全球最大的死因,也是心力衰竭(HF)最常见的病因。由于人口老龄化以及对心肌梗死等既往致命疾病的急性心脏护理有所改善,HF的发病率和患病率正在上升。迫切需要改善缺血性收缩性HF患者预后的策略。HF患者对冠状动脉疾病检测的系统性利用不足,尽管在缺血性心力衰竭扩展研究的外科治疗中,有证据表明冠状动脉旁路移植术(CABG)比药物治疗能降低死亡率,但接受血运重建的患者比例更小。经皮冠状动脉介入治疗(PCI)是一种侵入性较小的冠状动脉血运重建方法;然而,最近的缺血性心室功能障碍血运重建(REVIVED)-英国心血管介入学会(BCIS2)试验未能证明PCI在缺血性收缩性HF患者中比药物治疗更具优势。PCI和CABG对缺血性收缩性HF患者的相对有效性仍然未知,尤其是在当代药物治疗时代。在本综述中,我们讨论了CABG在缺血性收缩性HF中的益处、其利用不足以及未满足的临床需求。我们还回顾了最近比较PCI与药物治疗的REVIVED-BCIS2试验,以及即将开展的针对缺血性收缩性HF的PCI随机对照试验,以及尽管正在进行的试验有望提供数据,但仍将存在的持续证据空白。在当代血运重建方法和药物治疗时代,仍需要有足够样本量的随机对照试验来确定PCI与CABG在缺血性收缩性HF中的相对临床有效性,以及针对射血分数保留的HF患者或左心室收缩功能障碍较轻形式患者的冠状动脉血运重建试验。