Tarhini Ahmad, Ghate Sameer R, Ionescu-Ittu Raluca, Manceur Ameur M, Ndife Briana, Jacques Philippe, Laliberté François, Nakasato Antonio, Burne Rebecca, Duh Mei Sheng
Department of Hematology and Medical Oncology, Cleveland Clinic, Taussig Cancer Center, Cleveland, Ohio.
Department of US Oncology HEOR, Novartis Pharmaceuticals Corporation, East Hanover, New Jersey.
Melanoma Res. 2018 Dec;28(6):618-628. doi: 10.1097/CMR.0000000000000507.
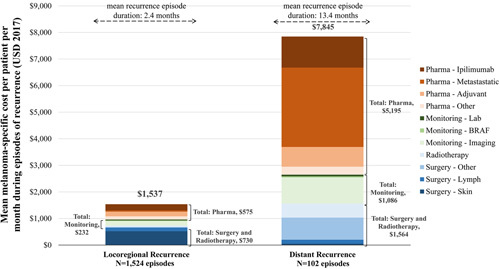
Surgery is the mainstay treatment for operable nonmetastatic melanoma, but recurrences are common and limit patients' survival. This study aimed to describe real-world patterns of treatment and recurrence in patients with melanoma and to quantify healthcare resource utilization (HRU) and costs associated with episodes of locoregional/distant recurrences. Adults with nonmetastatic melanoma who underwent melanoma lymph node surgery were identified from the Truven Health MarketScan database (1 January 2008 to 31 July 2017). Locoregional and distant recurrence(s) were identified on the basis of postsurgery recurrence indicators (i.e. initiation of new melanoma pharmacotherapy, new radiotherapy, or new surgery; secondary malignancy diagnoses). Of 6400 eligible patients, 219 (3.4%) initiated adjuvant therapy within 3 months of surgery, mostly with interferon α-2b (n=206/219, 94.1%). A total of 1191/6400 (18.6%) patients developed recurrence(s) over a median follow-up of 23.1 months (102/6400, 1.6% distant recurrences). Among the 219 patients initiated on adjuvant therapy, 73 (33.3%) experienced recurrences (distant recurrences: 13/219, 5.9%). The mean total all-cause healthcare cost was $2645 per patient per month (PPPM) during locoregional recurrence episodes and $12 940 PPPM during distant recurrence episodes. In the year after recurrence, HRU was particularly higher in patients with distant recurrence versus recurrence-free matched controls: by 9.2 inpatient admissions, 54.4 inpatient days, 8.8 emergency department admissions, and 185.9 outpatient visits (per 100 person-months), whereas all-cause healthcare costs were higher by $14 953 PPPM. It remains to be determined whether the new generation of adjuvant therapies, such as immune checkpoint inhibitors and targeted agents, will increase the use of adjuvant therapies, and reduce the risk of recurrences and associated HRU/cost.
手术是可手术切除的非转移性黑色素瘤的主要治疗方法,但复发很常见,会限制患者的生存。本研究旨在描述黑色素瘤患者的真实世界治疗和复发模式,并量化与局部/远处复发事件相关的医疗资源利用(HRU)和成本。从Truven Health MarketScan数据库(2008年1月1日至2017年7月31日)中确定接受黑色素瘤淋巴结手术的非转移性黑色素瘤成年患者。根据术后复发指标(即开始新的黑色素瘤药物治疗、新的放射治疗或新的手术;继发性恶性肿瘤诊断)确定局部和远处复发情况。在6400名符合条件的患者中,219名(3.4%)在术后3个月内开始辅助治疗,主要使用α-2b干扰素(n=206/219,94.1%)。在中位随访23.1个月期间,共有1191/6400名(18.6%)患者出现复发(102/6400名,1.6%为远处复发)。在开始辅助治疗的219名患者中,73名(33.3%)出现复发(远处复发:13/219,5.9%)。局部复发期间每位患者每月的全因医疗费用平均为2645美元,远处复发期间为12940美元。复发后的一年里,远处复发患者的HRU明显高于无复发的匹配对照组:住院入院多9.2次、住院天数多54.4天、急诊科就诊多8.8次、门诊就诊多185.9次(每100人月),而全因医疗费用高出14953美元。新一代辅助治疗,如免疫检查点抑制剂和靶向药物,是否会增加辅助治疗的使用,并降低复发风险以及相关的HRU/成本,仍有待确定。