Girerd S, Schikowski J, Girerd N, Duarte K, Busby H, Gambier N, Ladrière M, Kessler M, Frimat L, Aarnink A
Service de Néphrologie et Transplantation rénale, CHRU Nancy Brabois, Vandoeuvre-les-, Nancy, France.
INSERM, Centre d'Investigations Cliniques Plurithématique 1433, Université de Lorraine, CHRU de Nancy and F-CRIN INI-CRCT, Nancy, France.
BMC Nephrol. 2018 Sep 15;19(1):232. doi: 10.1186/s12882-018-1014-2.
In low-immunological risk kidney transplant recipients (KTRs), reduced exposure to calcineurin inhibitor (CNI) appears particularly attractive for avoiding adverse events, but may increase the risk of developing de novo Donor Specific Antibodies (dnDSA).
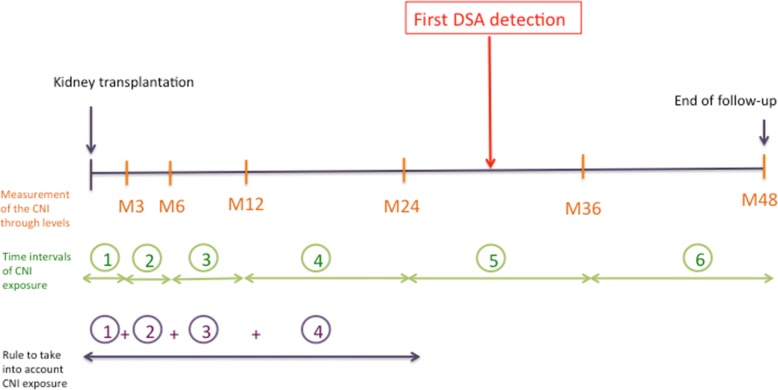
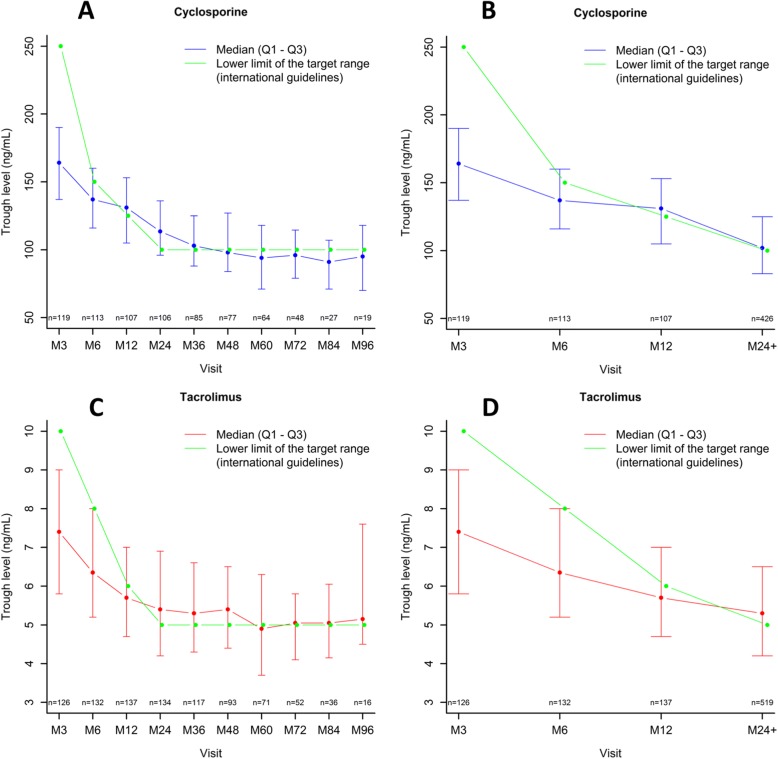
CNI exposure was retrospectively analyzed in 247 non-HLA immunized first KTRs by taking into account trough levels (C0) collected during follow-up. Reduced exposure to CNI was defined as follows: C0 less than the lower limit of the international targets for ≥50% of follow-up.
During a mean follow-up of 5.0 ± 2.0 years, 39 patients (15.8%) developed dnDSA (MFI ≥1000). Patients with DSA were significantly younger (46.6 ± 13.8 vs. 51.7 ± 14.0 years, p = 0.039), received more frequently poorly-matched grafts (59% with 6-8 A-B-DR-DQ HLA mismatches vs. 34.6%, p = 0.016) and had more frequently a reduced exposure to CNI (92.3% vs. 62.0%, p = 0.0002). Reduced exposure to CNI was associated with an increased risk of dnDSA (multivariable HR = 9.77, p = 0.002). Reduced exposure to CNI had no effect on patient survival, graft loss from any cause including death, or post-transplant cancer.
Even in a low-immunological risk population, reduced exposure to CNI is associated with increased risk of dnDSA. Benefits and risks of under-immunosuppression must be carefully evaluated before deciding on CNI minimization.
在低免疫风险的肾移植受者(KTR)中,减少钙调神经磷酸酶抑制剂(CNI)的暴露对于避免不良事件似乎特别有吸引力,但可能会增加新发供者特异性抗体(dnDSA)的风险。
对247例非HLA免疫的初次肾移植受者的CNI暴露情况进行回顾性分析,考虑随访期间收集的谷值水平(C0)。将减少CNI暴露定义如下:C0低于国际目标下限的时间≥随访时间的50%。
在平均5.0±2.0年的随访期间,39例患者(15.8%)出现dnDSA(平均荧光强度≥1000)。发生DSA的患者明显更年轻(46.6±13.8岁 vs. 51.7±14.0岁,p = 0.039),更频繁地接受配型不佳的移植物(59%的患者有6 - 8个A - B - DR - DQ HLA错配,而34.6%的患者无错配,p = 0.016),并且更频繁地减少CNI暴露(92.3% vs. 62.0%,p = 0.0002)。减少CNI暴露与dnDSA风险增加相关(多变量风险比 = 9.77,p = 0.002)。减少CNI暴露对患者生存率、包括死亡在内的任何原因导致的移植物丢失或移植后癌症均无影响。
即使在低免疫风险人群中,减少CNI暴露也与dnDSA风险增加相关。在决定最小化CNI之前,必须仔细评估免疫抑制不足的益处和风险。