Division of Gastroenterology and Hepatology, Medical College of Georgia, Augusta University, Augusta, GA, USA; Department of Medicine, University of Iowa Carver College of Medicine, Iowa City, IA, USA.
Department of Medicine, University of Iowa Carver College of Medicine, Iowa City, IA, USA.
Lancet Gastroenterol Hepatol. 2018 Nov;3(11):768-777. doi: 10.1016/S2468-1253(18)30266-8. Epub 2018 Sep 18.
Office-based biofeedback therapy is effective for constipation with dyssynergic defecation, but must be performed by skilled staff, is only available in selected centres, and requires multiple visits. The efficacy of home-based biofeedback therapy is unknown. We compared clinical and subjective outcomes with home-based and office-based approaches.
In this randomised controlled trial, eligible patients were adult outpatients (age 18-80 years) who met the Rome III criteria for functional constipation and who had been referred to a tertiary-care centre after non-response to routine management, and who had dyssynergic defecation. Patients were randomly assigned according to a schedule generated in advance by the study biostatistician, in permuted blocks of four, to receive office-based or home-based biofeedback therapy. Office-based biofeedback comprised therapist-guided pelvic floor training for six sessions over 3 months (visits every 2 weeks). Home-based biofeedback comprised 20 min self-training sessions twice per day, in which a self-inserted probe was used to provide visual feedback via a handheld monitoring device of anal sphincter pressure and push effort. Patients recorded in diaries the time of each defecation attempt, stool consistency, straining effort, feeling of incomplete evacuation, need for digital assistance with stooling, and satisfaction with bowel function, from 1 week before enrolment to the end of follow-up. Treatment responders were defined post hoc as those with normalisation of dyssynergic defecation and an increase in the number of complete spontaneous bowel movements per week by 3 months. Cost outcomes calculated from health-care costs and loss of salary were assessed from hospital billing and medical records and questionnaires. Primary outcome measures were the presence of a dyssynergic pattern during attempted defecation, balloon expulsion time, the number of complete spontaneous bowel movements per week, and satisfaction with bowel function, assessed by intention to treat (non-inferiority) and per protocol. This trial is registered with ClinicalTrials.gov, number NCT03202771.
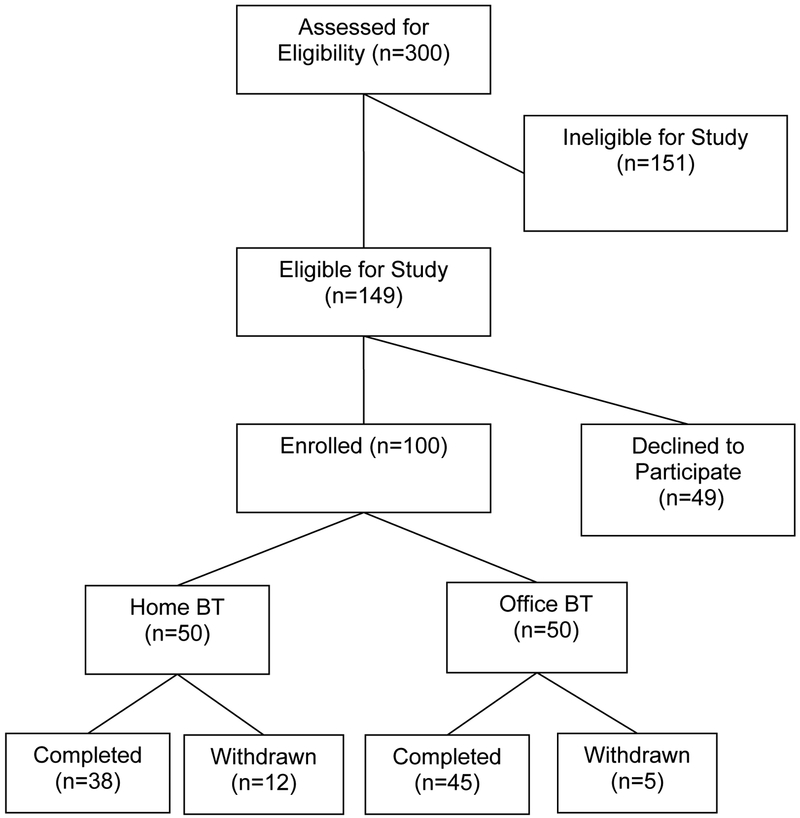
Of 300 patients screened we enrolled 100, from Jan 7, 2005, to Jan 31, 2010. 83 patients completed training (38 [76%] of 50 in the home-based biofeedback group and 45 [90%] of 50 in the office-based biofeedback group). 34 (68%) patients in the home-based group and 35 (70%) in the office-based group were classified as responders. All primary outcomes improved significantly from baseline in the two treatment groups (all p<0·0001). Home-based biofeedback therapy was non-inferior to office-based therapy for number of complete spontaneous bowel movements per week, satisfaction with bowel function, and balloon expulsion time in the intention-to-treat and per-protocol analyses, and for dyssynergia in the per-protocol analysis. No adverse events were reported. The median cost of home-based biofeedback therapy was significantly lower than that for office-based treatment (US$1081·70, IQR 794·90-1399·30 vs $1942·50, 1621·70-2369·00, p=0·009).
Home-based and office-based biofeedback therapy for dyssynergic defecation improved bowel symptoms and physiology with similar efficacy. A home-based programme could substantially broaden the availability and use of this treatment.
National Institutes of Health.
对于伴有功能性出口梗阻的便秘患者,基于诊室的生物反馈治疗有效,但必须由熟练的医护人员操作,仅在部分中心开展,且需要多次就诊。家庭为基础的生物反馈治疗的疗效尚不清楚。我们比较了基于诊室和家庭两种方法的临床和主观疗效。
在这项随机对照试验中,合格的患者为成年门诊患者(年龄 18-80 岁),符合罗马 III 功能性便秘标准,在常规治疗无反应后被转诊至三级医疗中心,并且存在功能性出口梗阻。患者根据研究生物统计学家预先制定的时间表,按 4 个患者为一组的顺序进行随机分组,接受基于诊室或家庭的生物反馈治疗。基于诊室的生物反馈包括治疗师指导的骨盆底训练,共 6 次,持续 3 个月(每 2 周就诊一次)。家庭为基础的生物反馈包括每天两次 20 分钟的自我训练,在此过程中,一个自插入的探头用于通过手持监测设备提供肛门括约肌压力和推力的视觉反馈。患者从入组前 1 周开始,至随访结束时,每天记录每次排便尝试的时间、粪便稠度、用力程度、不完全排空感、排便时需要数字辅助的感觉,以及对排便功能的满意度。治疗应答者定义为:在 3 个月时,通过异常的肛门直肠动力学改善和每周完全自发性排便次数增加 3 次。从医院账单和医疗记录以及问卷调查中评估医疗保健费用和工资损失的成本结果。主要结局指标为尝试排便时存在的异常肛门直肠动力学模式、球囊排出时间、每周完全自发性排便次数以及基于意向治疗(非劣效性)和方案的排便功能满意度。这项试验在 ClinicalTrials.gov 注册,编号为 NCT03202771。
在筛选的 300 名患者中,我们纳入了 100 名患者,纳入时间为 2005 年 1 月 7 日至 2010 年 1 月 31 日。83 名患者完成了训练(50 名家庭为基础的生物反馈组中 38 名[76%],50 名基于诊室的生物反馈组中 45 名[90%])。家庭为基础的生物反馈组中 34 名(68%)患者和基于诊室的生物反馈组中 35 名(70%)患者被分类为应答者。两组患者的所有主要结局指标均较基线显著改善(所有 p<0·0001)。基于意向治疗和方案的分析,家庭为基础的生物反馈治疗在每周完全自发性排便次数、排便功能满意度和球囊排出时间方面不劣于基于诊室的治疗,而在方案分析中,家庭为基础的生物反馈治疗在异常肛门直肠动力学方面不劣于基于诊室的治疗。未报告不良事件。家庭为基础的生物反馈治疗的中位费用明显低于基于诊室的治疗(1081.70 美元,794.90-1399.30 美元 vs 1942.50 美元,1621.70-2369.00 美元,p=0·009)。
对于伴有功能性出口梗阻的便秘患者,基于诊室的生物反馈治疗和家庭为基础的生物反馈治疗均可改善肠道症状和生理功能,疗效相当。家庭为基础的方案可以显著扩大这种治疗的可及性和使用范围。
美国国立卫生研究院。