PhyMedExp, University of Montpellier, Anesthesiology and Intensive Care; Anesthesia and Critical Care Department B, Saint Eloi Teaching Hospital, Centre Hospitalier Universitaire Montpellier, 34295, Montpellier, cedex 5, France.
Université Cote d'Azur, CNRS U7275, CHU de Nice, Service réanimation polyvalente et U 7275, IPMC, Nice, France.
Crit Care. 2018 Sep 23;22(1):236. doi: 10.1186/s13054-018-2150-6.
Patients liberated from invasive mechanical ventilation are at risk of extubation failure, including inability to breathe without a tracheal tube (airway failure) or without mechanical ventilation (non-airway failure). We sought to identify respective risk factors for airway failure and non-airway failure following extubation.
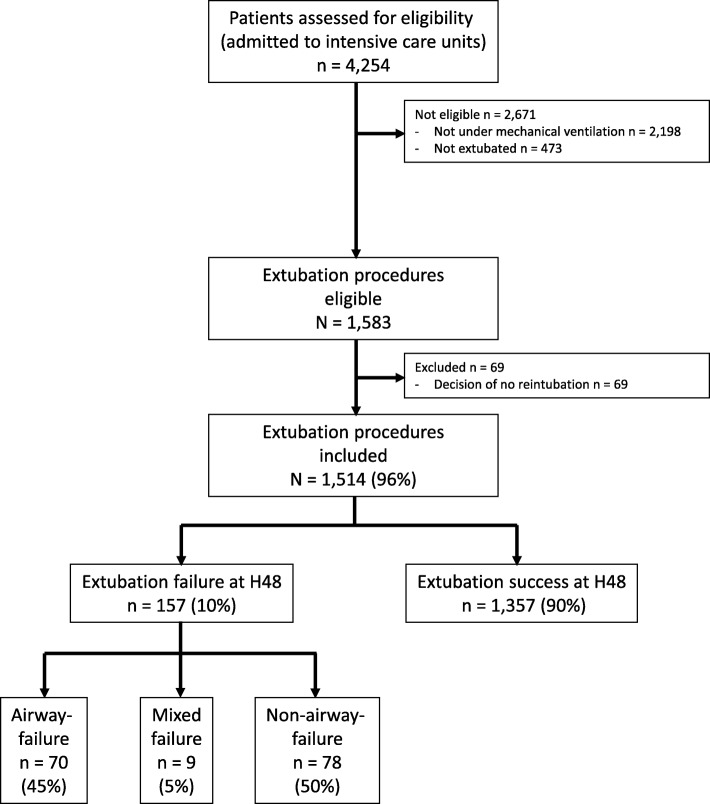
The primary endpoint of this prospective, observational, multicenter study in 26 intensive care units was extubation failure, defined as need for reintubation within 48 h following extubation. A multinomial logistic regression model was used to identify risk factors for airway failure and non-airway failure.
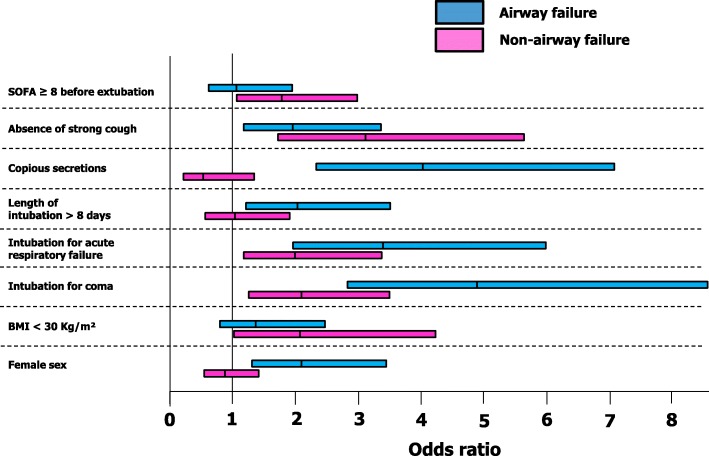
Between 1 December 2013 and 1 May 2015, 1514 patients undergoing extubation were enrolled. The extubation-failure rate was 10.4% (157/1514), including 70/157 (45%) airway failures, 78/157 (50%) non-airway failures, and 9/157 (5%) mixed airway and non-airway failures. By multivariable analysis, risk factors for extubation failure were either common to airway failure and non-airway failure: intubation for coma (OR 4.979 (2.797-8.864), P < 0.0001 and OR 2.067 (1.217-3.510), P = 0.003, respectively, intubation for acute respiratory failure (OR 3.395 (1.877-6.138), P < 0.0001 and OR 2.067 (1.217-3.510), P = 0.007, respectively, absence of strong cough (OR 1.876 (1.047-3.362), P = 0.03 and OR 3.240 (1.786-5.879), P = 0.0001, respectively, or specific to each specific mechanism: female gender (OR 2.024 (1.187-3.450), P = 0.01), length of ventilation > 8 days (OR 1.956 (1.087-3.518), P = 0.025), copious secretions (OR 4.066 (2.268-7.292), P < 0.0001) were specific to airway failure, whereas non-obese status (OR 2.153 (1.052-4.408), P = 0.036) and sequential organ failure assessment (SOFA) score ≥ 8 (OR 1.848 (1.100-3.105), P = 0.02) were specific to non-airway failure. Both airway failure and non-airway failure were associated with ICU mortality (20% and 22%, respectively, as compared to 6% in patients with extubation success, P < 0.0001).
Specific risk factors have been identified, allowing us to distinguish between risk of airway failure and non-airway failure. The two conditions will be managed differently, both for prevention and curative strategies.
ClinicalTrials.gov, NCT 02450669 . Registered on 21 May 2015.
从有创机械通气中解放出来的患者有发生拔管失败的风险,包括无气管插管(气道失败)或无机械通气(非气道失败)时无法呼吸。我们试图确定拔管后气道失败和非气道失败的各自危险因素。
这项前瞻性、观察性、多中心研究在 26 个重症监护病房进行,主要终点为拔管后 48 小时内需要再次插管的拔管失败。采用多项逻辑回归模型确定气道失败和非气道失败的危险因素。
2013 年 12 月 1 日至 2015 年 5 月 1 日,共纳入 1514 例接受拔管的患者。拔管失败率为 10.4%(157/1514),其中 70/157(45%)为气道失败,78/157(50%)为非气道失败,9/157(5%)为混合气道和非气道失败。多变量分析显示,拔管失败的危险因素既有气道失败又有非气道失败的共同危险因素:昏迷插管(OR 4.979(2.797-8.864),P<0.0001 和 OR 2.067(1.217-3.510),P=0.003),急性呼吸衰竭插管(OR 3.395(1.877-6.138),P<0.0001 和 OR 2.067(1.217-3.510),P=0.007),无强烈咳嗽(OR 1.876(1.047-3.362),P=0.03 和 OR 3.240(1.786-5.879),P=0.0001),或每个特定机制的特定危险因素:女性(OR 2.024(1.187-3.450),P=0.01),通气时间>8 天(OR 1.956(1.087-3.518),P=0.025),大量分泌物(OR 4.066(2.268-7.292),P<0.0001)是气道失败的特定危险因素,而非肥胖状态(OR 2.153(1.052-4.408),P=0.036)和序贯器官衰竭评估(SOFA)评分≥8(OR 1.848(1.100-3.105),P=0.02)是非气道失败的特定危险因素。气道失败和非气道失败均与 ICU 死亡率相关(分别为 20%和 22%,而拔管成功患者的死亡率为 6%,P<0.0001)。
已经确定了特定的危险因素,使我们能够区分气道失败和非气道失败的风险。这两种情况的预防和治疗策略都将有所不同。
ClinicalTrials.gov,NCT 02450669。于 2015 年 5 月 21 日注册。