Danos Denise, Leonardi Claudia, Gilliland Aubrey, Shankar Sharmila, Srivastava Rakesh K, Simonsen Neal, Ferguson Tekeda, Yu Qingzhao, Wu Xiao-Cheng, Scribner Richard
Louisiana State University Health Sciences Center School of Medicine, Stanley S. Scott Cancer Center, New Orleans, LA, United States.
Behavioral and Community Health Sciences Department, Louisiana State University Health Sciences Center School of Public Health, New Orleans, LA, United States.
Front Oncol. 2018 Sep 11;8:375. doi: 10.3389/fonc.2018.00375. eCollection 2018.
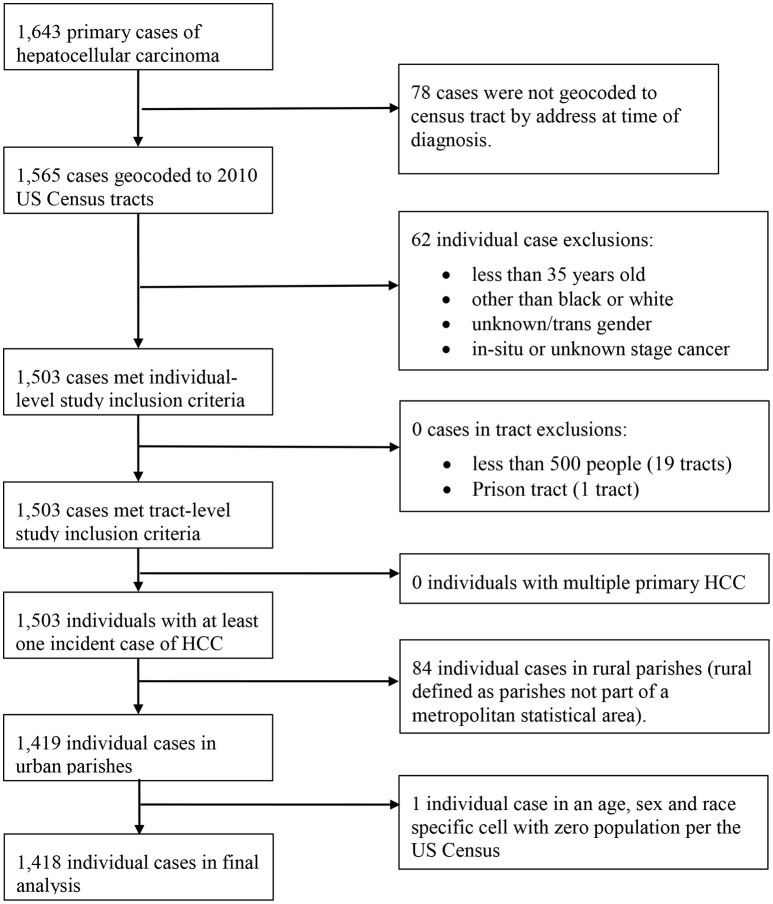
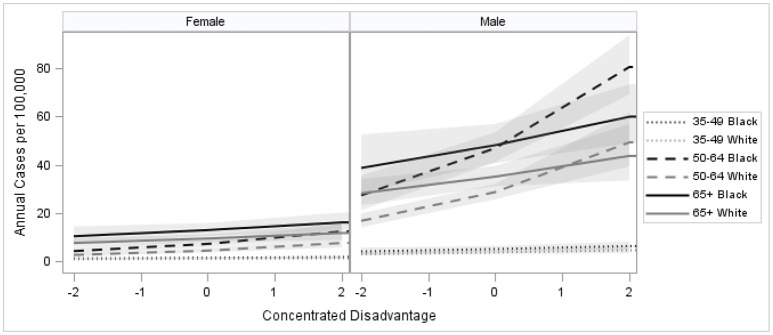
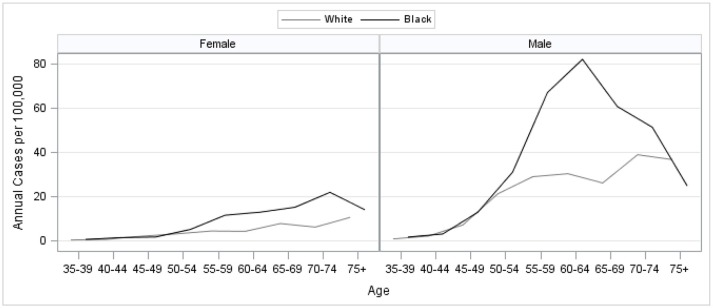
Over the past three decades, Hepatocellular Carcinoma (HCC) is one of few cancers for which incidence has increased in the United States (US). It is likely social determinants at the population level are driving this increase. We designed a population-based study to explore whether social determinants at the neighborhood level are geographically associated with HCC incidence in Louisiana by examining the association of HCC incidence with neighborhood concentrated disadvantage. Primary HCC cases diagnosed from 2008 to 2012 identified from the Louisiana Tumor Registry were geocoded to census tract of residence at the time of diagnosis. Neighborhood concentrated disadvantage index (CDI) for each census tract was calculated according to the PhenX Toolkit data protocol based on population and socioeconomic measures from the US Census. The incidence of HCC was modeled using multilevel binomial regression with individuals nested within neighborhoods. The study included 1,418 HCC cases. Incidence of HCC was greater among males than females and among black than white. In multilevel models controlling for age, race, and sex, neighborhood CDI was positively associated with the incidence of HCC. A one standard deviation increase in CDI was associated with a 22% increase in HCC risk [Risk Ratio (RR) = 1.22; 95% CI (1.15, 1.31)]. Adjusting for contextual effects of an individual's neighborhood reduced the disparity in HCC incidence. Neighborhood concentrated disadvantage, a robust measure of an adverse social environment, was found to be a geographically associated with HCC incidence. Differential exposure to neighborhoods characterized by concentrated disadvantage partially explained the racial disparity in HCC for Louisiana. Our results suggest that increasing rates of HCC, and existing racial disparities for the disease, are partially explained by measures of an adverse social environment.
在过去三十年里,肝细胞癌(HCC)是美国发病率有所上升的少数几种癌症之一。很可能是人群层面的社会决定因素推动了这一增长。我们设计了一项基于人群的研究,通过检查HCC发病率与邻里集中劣势之间的关联,来探究邻里层面的社会决定因素在地理上是否与路易斯安那州的HCC发病率相关。从路易斯安那肿瘤登记处识别出的2008年至2012年诊断的原发性HCC病例,在诊断时被地理编码到居住的普查区。根据PhenX工具包数据协议,基于美国人口普查的人口和社会经济指标,计算每个普查区的邻里集中劣势指数(CDI)。使用个体嵌套在邻里中的多级二项回归对HCC发病率进行建模。该研究包括1418例HCC病例。HCC的发病率在男性中高于女性,在黑人中高于白人。在控制年龄、种族和性别的多级模型中,邻里CDI与HCC发病率呈正相关。CDI增加一个标准差与HCC风险增加22%相关[风险比(RR)=1.22;95%置信区间(1.15,1.31)]。调整个体邻里的背景效应可减少HCC发病率的差异。邻里集中劣势是对不利社会环境的一种有力衡量指标,被发现与HCC发病率在地理上相关。对以集中劣势为特征的邻里的不同暴露,部分解释了路易斯安那州HCC的种族差异。我们的结果表明,HCC发病率的上升以及该疾病现有的种族差异,部分可由不利社会环境的指标来解释。