Divisions of Gastroenterology and Hepatology, William J. von Liebig Transplant Center, Mayo Clinic, Rochester, MN.
Department of Radiology, Mayo Clinic, Rochester, MN.
Liver Transpl. 2019 Jan;25(1):14-24. doi: 10.1002/lt.25346.
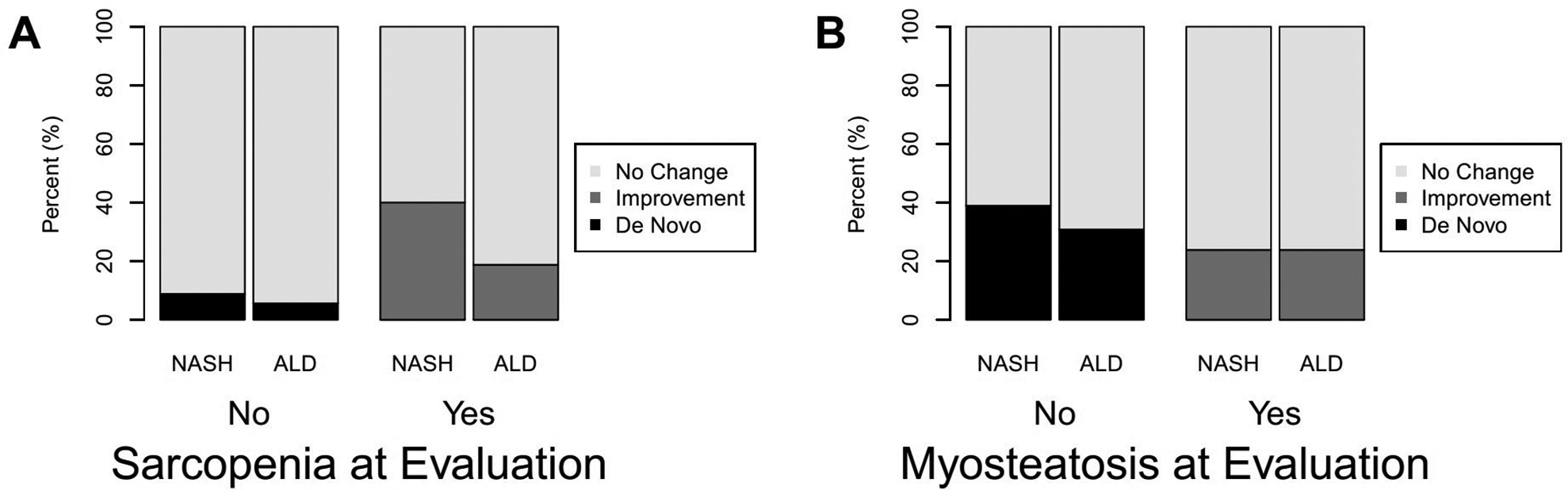
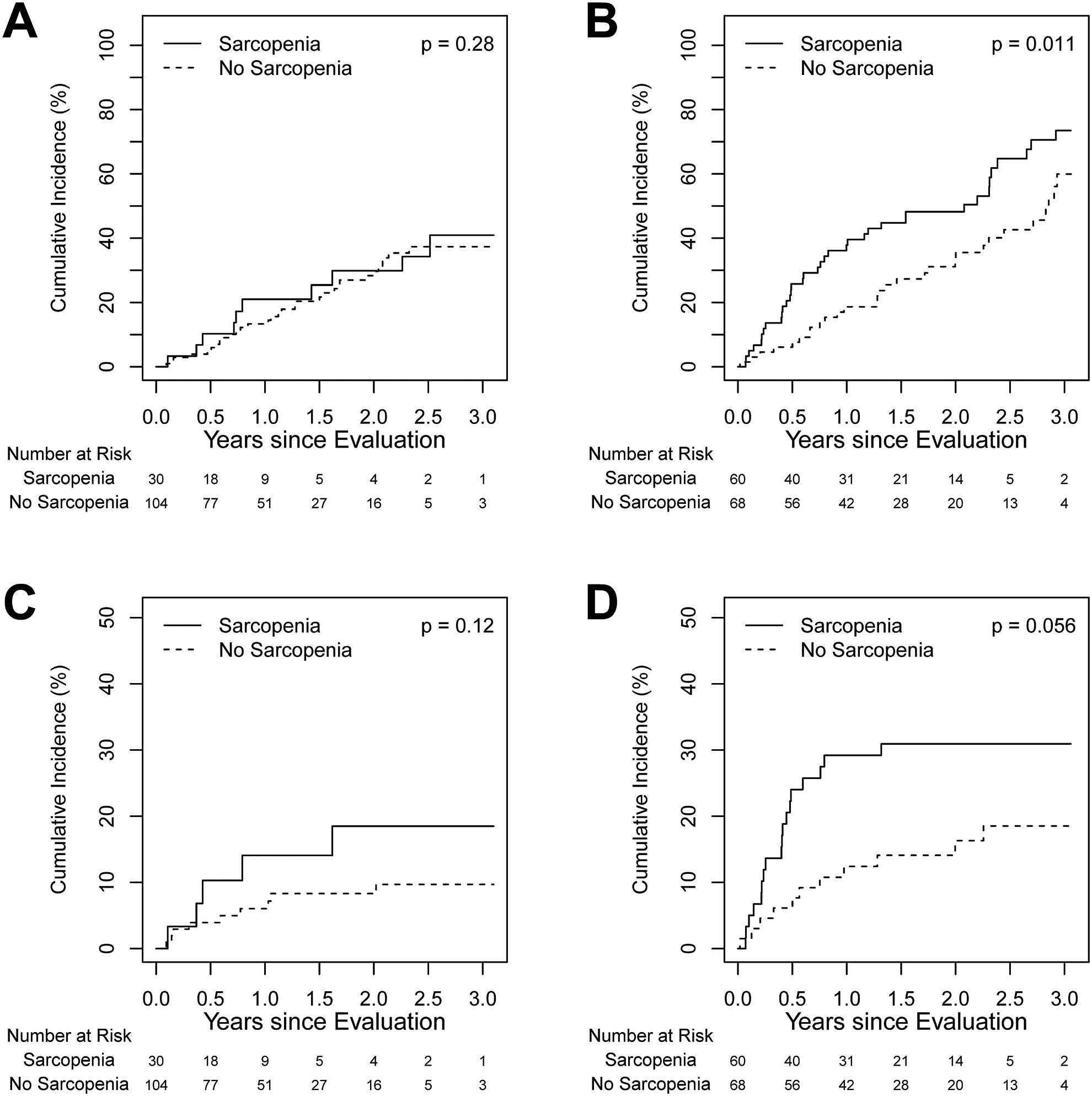
Sarcopenia and frailty are commonly encountered in patients with end-stage liver disease and are associated with adverse clinical outcomes, including decompensation and wait-list mortality. The impact of these entities in patients with differing disease etiologies has not been elucidated. We aim to ascertain the change in their prevalence over time on the wait list and determine their impact on hospitalization, delisting, and wait-list survival, specifically for patients with nonalcoholic steatohepatitis (NASH) and alcoholic liver disease (ALD). Adult patients who were evaluated for their first liver transplant from 2014 to 2016 with a primary diagnosis of NASH (n = 136) or ALD (n = 129) were included. Computed tomography scans were used to determine the presence of sarcopenia and myosteatosis. Frailty was diagnosed using the Rockwood frailty index. Patients with NASH had a significantly lower prevalence of sarcopenia (22% versus 47%; P < 0.001) but a significantly higher prevalence of frailty (49% versus 34%; P = 0.03) when compared with patients with ALD at the time of listing. In patients with NASH, sarcopenia was not associated with adverse events, but a higher frailty score was associated with an increased length of hospitalization (P = 0.05) and an increased risk of delisting (P = 0.02). In patients with ALD, univariate analysis showed the presence of sarcopenia was associated with an increased risk of delisting (P = 0.01). In conclusion, sarcopenia and frailty occur with differing prevalence with variable impact on outcomes in wait-listed patients with NASH and ALD.
肌肉减少症和虚弱在终末期肝病患者中很常见,与不良临床结局相关,包括失代偿和等待名单死亡率。这些实体在不同病因的患者中的影响尚未阐明。我们旨在确定它们在等待名单上随时间的变化趋势,并确定它们对住院、取消资格和等待名单生存的影响,特别是对于非酒精性脂肪性肝炎 (NASH) 和酒精性肝病 (ALD) 患者。纳入了 2014 年至 2016 年期间因 NASH(n = 136)或 ALD(n = 129)接受首次肝移植评估的成年患者。使用计算机断层扫描确定存在肌肉减少症和肌内脂肪变性。使用 Rockwood 虚弱指数诊断虚弱。与 ALD 患者相比,NASH 患者在列入名单时肌肉减少症的患病率明显较低(22%对 47%;P < 0.001),但虚弱的患病率明显较高(49%对 34%;P = 0.03)。在 NASH 患者中,肌肉减少症与不良事件无关,但较高的虚弱评分与住院时间延长(P = 0.05)和取消资格风险增加(P = 0.02)相关。在 ALD 患者中,单因素分析显示肌肉减少症与取消资格风险增加相关(P = 0.01)。总之,肌肉减少症和虚弱在 NASH 和 ALD 等待名单患者中的发生率不同,对结局的影响也不同。