Sikdar Nilabja, Saha Gourab, Dutta Ashmita, Ghosh Shibajyoti, Shrikhande Shailesh V, Banerjee Sudeep
1Human Genetics Unit, Indian Statistical Institute, 203 B.T. Road, Kolkata 700108, West Bengal, India; 2Medical College and Hospital, 88, College Street, Kolkata 700073, West Bengal, India; 3Tata Memorial Centre, Mumbai400012, India; 4Tata Medical Center, Newtown, Rajarhat, 700156, Kolkata, West Bengal, India.
Curr Genomics. 2018 Sep;19(6):444-463. doi: 10.2174/1389202919666180221160753.
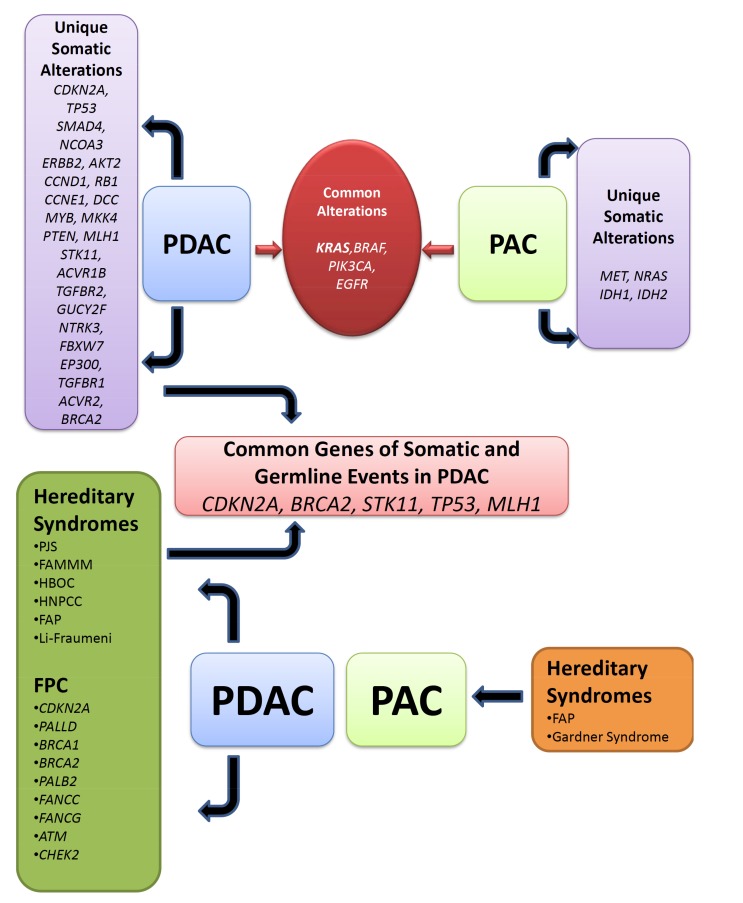
Pancreatic Ductal AdenoCarcinoma (PDAC) is one of the most lethal malignancies of all solid cancers. Precancerous lesions for PDAC include PanIN, IPMNs and MCNs. PDAC has a poor prognosis with a 5-year survival of approximately 6%. Whereas Periampulary AdenoCarcinoma (PAC) having four anatomic subtypes, pancreatic, Common Bile Duct (CBD), ampullary and duodenum shows relative better prognosis. The highest incidence of PDAC has been reported with black with respect to white population. Similarly, incidence rate of PAC also differs with different ethnic populations. Several lifestyle, environmental and occupational exposures including long-term diabetes, obesity, and smoking, have been linked to PDAC, however, for PAC the causal risk factors were poorly described. It is now clear that PDAC and PAC are a multi-stage process resulting from the accumulation of genomic alterations in the somatic DNA of normal cells as well as inherited mutations. Approximately 10% of PDAC have a familial inheritance. Germline mutations in CDKN2A, BRCA2, STK11, PALB2, PRSS1, etc., as well as certain syndromes have been well associated with predisposition to PDAC. KRAS, CDKN2A, TP53 and SMAD4 are the 4 "mountains" (high-frequency driver genes) which have been known to earliest somatic alterations for PDAC while relatively less frequent in PAC. Our understanding of the molecular carcinogenesis has improved in the last few years due to extensive research on PDAC which was not well explored in case of PAC. The genetic alterations that have been identified in PDAC and different subgroups of PAC are important implications for the development of genetic screening test, early diagnosis, and prognostic genetic markers. The present review will provide a brief overview of the incidence and prevalence of PDAC and PAC, mainly, increased risk in India, the several kinds of risk factors associated with the diseases as well as required genetic alterations for disease initiation and progression.
胰腺导管腺癌(PDAC)是所有实体癌中致死率最高的恶性肿瘤之一。PDAC的癌前病变包括胰腺上皮内瘤变(PanIN)、导管内乳头状黏液性肿瘤(IPMN)和黏液性囊性肿瘤(MCN)。PDAC预后较差,5年生存率约为6%。而壶腹周围腺癌(PAC)有四种解剖学亚型,即胰腺型、胆总管型、壶腹型和十二指肠型,其预后相对较好。据报道,黑人中PDAC的发病率高于白人。同样,PAC的发病率在不同种族人群中也有所不同。包括长期糖尿病、肥胖和吸烟在内的几种生活方式、环境和职业暴露都与PDAC有关,然而,对于PAC,其因果风险因素描述较少。现在很清楚,PDAC和PAC是一个多阶段过程,是正常细胞体细胞DNA中基因组改变以及遗传突变积累的结果。大约10%的PDAC有家族遗传。细胞周期蛋白依赖性激酶2A(CDKN2A)、乳腺癌2号基因(BRCA2)、丝氨酸/苏氨酸蛋白激酶11(STK11)、乳腺癌2号基因伴侣蛋白(PALB2)、丝氨酸蛋白酶1(PRSS1)等基因的种系突变以及某些综合征与PDAC的易感性密切相关。KRAS、CDKN2A、TP53和SMAD4是4个“山峰”(高频驱动基因),已知它们是PDAC最早的体细胞改变,而在PAC中相对较少见。由于对PDAC进行了广泛研究,而PAC方面的研究较少,在过去几年中我们对分子致癌作用的理解有了提高。在PDAC和PAC不同亚组中发现的基因改变对基因筛查试验、早期诊断和预后遗传标志物的开发具有重要意义。本综述将简要概述PDAC和PAC的发病率和患病率,主要是印度的患病风险增加情况、与这些疾病相关的几种风险因素以及疾病发生和进展所需的基因改变。