Division of Pharmacy, College of Health and Medicine, University of Tasmania, Hobart, Tasmania, Australia.
Department of Anaesthesia, Launceston General Hospital, Launceston, Tasmania, Australia.
Obes Surg. 2019 Jan;29(1):159-165. doi: 10.1007/s11695-018-3497-0.
Most surgical prophylaxis guidelines recommend a 3-g cefazolin intravenous dose in patients weighing ≥ 120 kg. However, this recommendation is primarily based on pharmacokinetic studies rather than robust clinical evidence. This study aimed to compare the prevalence of surgical site infections (SSIs) in obese and non-obese patients (body mass index ≥ 30 kg/m and < 30 kg/m), and those weighing ≥ 120 kg and < 120 kg, who received 2- g cefazolin preoperatively.
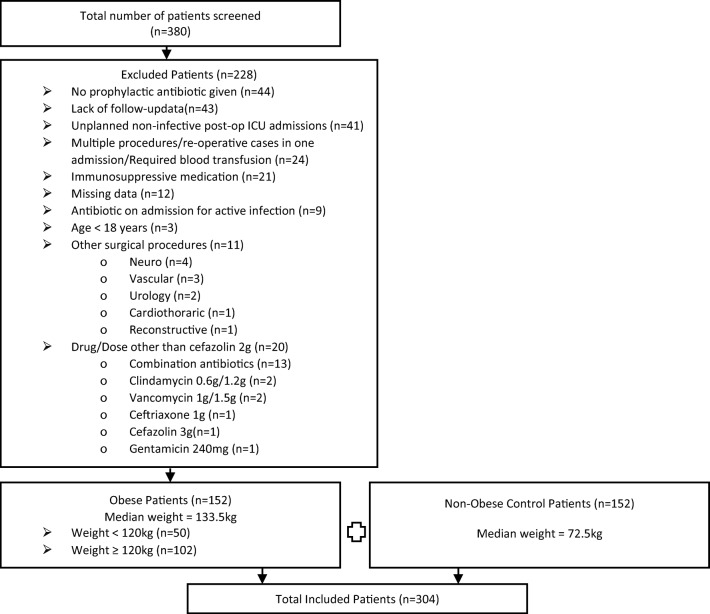
A retrospective case-control study was conducted in adult elective surgical patients. Patients receiving 2- g cefazolin were grouped as obese and non-obese, and by weight (≥ 120 kg or < 120 kg). The 90-day prevalence of SSI and potential contributing factors were investigated.
We identified 152 obese (median 134 kg) and 152 non-obese control (median 73 kg) patients. Baseline characteristics were similar between groups, except for an increased prevalence in the obese group of diabetes (35.5% vs 13.2%; p < 0.001) and an American Society of Anaesthesiologists Score of 3 (61.8% vs 17.1%; p < 0.001). While not statistically significant, the prevalence of SSI in the obese group was almost double that in the non-obese group (8.6% vs 4.6%; p = 0.25) and in patients weighing ≥ 120 kg (n = 102) compared to those weighing < 120 kg (n = 202) (9.8% vs 5.0%; p = 0.17).
The prevalence of SSI was not significantly increased in obese patients, or those weighing ≥ 120 kg, who received cefazolin 2- g prophylactically; however, trends toward an increase were evident. Large-scale randomised trials are needed to examine whether a 2-g or 3-g cefazolin is adequate to prevent SSI in obese (and ≥ 120 kg) individuals.
大多数外科预防指南建议体重≥120kg 的患者静脉注射 3g 头孢唑林。然而,这一建议主要基于药代动力学研究,而非确凿的临床证据。本研究旨在比较接受术前 2g 头孢唑林的肥胖患者(体重指数≥30kg/m2 且<30kg/m2)和非肥胖患者(体重指数<30kg/m2),以及体重≥120kg 和<120kg 的患者中手术部位感染(SSI)的发生率。
本研究采用回顾性病例对照研究,纳入成年择期手术患者。接受 2g 头孢唑林的患者分为肥胖组和非肥胖组,并根据体重(≥120kg 或<120kg)进行分组。调查 90 天内 SSI 的发生率和潜在的影响因素。
本研究共纳入 152 例肥胖患者(中位体重 134kg)和 152 例非肥胖对照组患者(中位体重 73kg)。两组患者的基线特征相似,但肥胖组糖尿病的发生率较高(35.5% vs 13.2%;p<0.001),美国麻醉医师协会评分≥3 级的患者比例较高(61.8% vs 17.1%;p<0.001)。尽管无统计学意义,但肥胖组 SSI 的发生率几乎是非肥胖组的两倍(8.6% vs 4.6%;p=0.25),体重≥120kg 的患者(n=102)与体重<120kg 的患者(n=202)相比(9.8% vs 5.0%;p=0.17)也偏高。
接受 2g 头孢唑林预防性治疗的肥胖患者或体重≥120kg 的患者,SSI 的发生率并未显著增加,但存在增加的趋势。需要开展大规模随机试验来研究头孢唑林 2g 或 3g 是否足以预防肥胖(和≥120kg)人群的 SSI。