Orthopedic Research Unit, Department of Orthopedic Surgery and Traumatology, Turku University Hospital and University of Turku, Turku, Finland.
J Orthop Res. 2019 Jan;37(1):239-247. doi: 10.1002/jor.24150. Epub 2018 Oct 25.
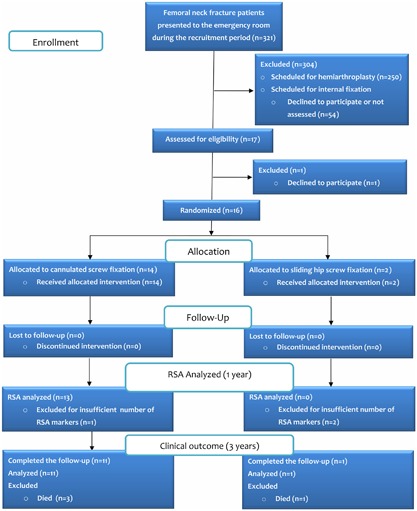
We examined the feasibility of radiostereometric analysis (RSA) in the assessment of the initial stability of internally fixed femoral neck fractures. The study included 16 patients (mean age 73 years). During surgery, multiple RSA-beads were inserted on both sides of the fracture. Radiographs for RSA were taken in the supine position within the first 3 days and 6, 12, 24, and 52 weeks after surgery. To detect any inducible motion at the fracture-site, radiographs for RSA were taken with the patient resting or applying a load through the fracture. Fracture loading was achieved by the patient pressing the ipsilateral foot as much as tolerated on a force plate while providing a counterforce through both hands. Micromotion exceeding the precision values of RSA (≥0.3 mm for the translation vector and/or ≥1.2 degrees for the rotation vector) was considered significant. Permanent three-dimensional fracture-site displacement was also recorded. Voluntary loading induced fracture-site micromotion, which exhibited a dichotomous distribution. In patients with uncomplicated fracture union, inducible micromotion was detectable only at baseline-if at all. Conversely, fractures that developed a nonunion were characterized by the continuation of inducible micromotion beyond baseline. Permanent fracture-site displacement was, on average, nearly an order of magnitude greater than the inducible micromotion. Fracture unions were characterized by the cessation of permanent fracture-site displacement by 12 weeks. Nonunions presented as outliers in permanent fracture-site displacement. Large-scale studies are warranted to evaluate whether the detection of inducible micromotion beyond baseline could serve as an indicator of insufficient fixation stability. © 2018 The Authors. Journal of Orthopaedic Research® Published by Wiley Periodicals, Inc. on behalf of the Orthopaedic Research Society.
我们研究了放射立体测量分析(RSA)在评估内置固定股骨颈骨折初始稳定性中的可行性。该研究纳入 16 名患者(平均年龄 73 岁)。手术时,在骨折两侧插入多个 RSA 珠。术后第 3 天内及 6、12、24 和 52 周时,患者仰卧位拍摄 RSA 射线片。为了检测骨折部位是否存在可诱导运动,在患者休息或通过骨折施加负荷时拍摄 RSA 射线片。骨折加载通过患者在力板上尽可能地按压对侧脚来实现,同时通过双手提供反向力。超过 RSA 精度值(平移矢量≥0.3mm 和/或旋转矢量≥1.2 度)的微运动被认为是显著的。还记录了永久性三维骨折部位位移。自愿负重引起的骨折部位微运动呈二分分布。在骨折愈合无并发症的患者中,仅在基线时可检测到诱导微运动(如果有的话)。相反,发生骨折不愈合的骨折的特征是诱导微运动持续超过基线。平均而言,永久性骨折部位位移几乎比可诱导微运动大一个数量级。骨折愈合的特征是在 12 周时永久性骨折部位位移停止。骨折不愈合在永久性骨折部位位移上呈异常值。需要进行大规模研究来评估是否可以将基线以外的可诱导微运动检测作为固定稳定性不足的指标。© 2018 作者。由 Wiley 期刊出版公司代表骨科研究协会出版的《骨科研究杂志》。