Lawson Peter J, Moore Hunter B, Moore Ernest E, Gerich Mark E, Stettler Gregory R, Banerjee Anirban, Schulick Richard D, Nydam Trevor L
Department of Surgery, University of Colorado School of Medicine, Aurora, Colorado.
Department of Surgery, University of Colorado School of Medicine, Aurora, Colorado.
J Surg Res. 2018 Nov;231:54-61. doi: 10.1016/j.jss.2018.04.059. Epub 2018 Jun 8.
Elevated clot strength (maximum amplitude [MA]) measured by thrombelastography (TEG) is associated with thrombotic complications. However, it remains unclear how MA translates to thrombotic risks, as this measurement is independent of time, blood flow, and clot degradation. We hypothesize that under flow conditions, increased clot strength correlates to time-dependent measurements of coagulation and resistance to fibrinolysis.
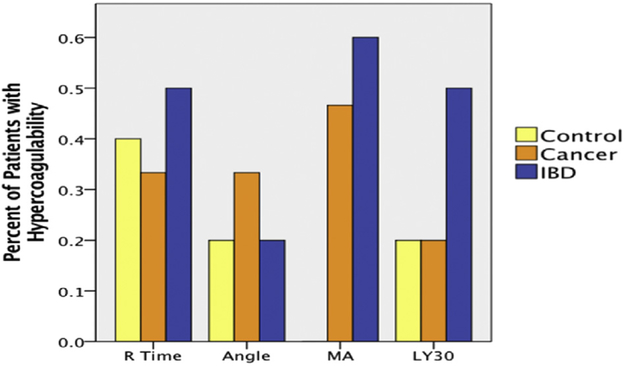
Surgical patients at high risk of thrombotic complications were analyzed with TEG and total thrombus-formation analysis system (T-TAS). TEG hypercoagulability was defined as an r <10.2 min, angle >59, MA >66 or LY30 <0.2% (based off of healthy control data, n = 141). The T-TAS AR and PL chips were used to measure clotting at arterial shear rates. T-TAS measurements include occlusion start time, occlusion time (OT), occlusion speed (OSp), and total clot generation (area under the curve). These measurements were correlated to TEG indices (R time, angle, MA, and LY30). Both T-TAS and TEG assays were challenged with tissue plasminogen activator (t-PA) to assess clot resistance to fibrinolysis.
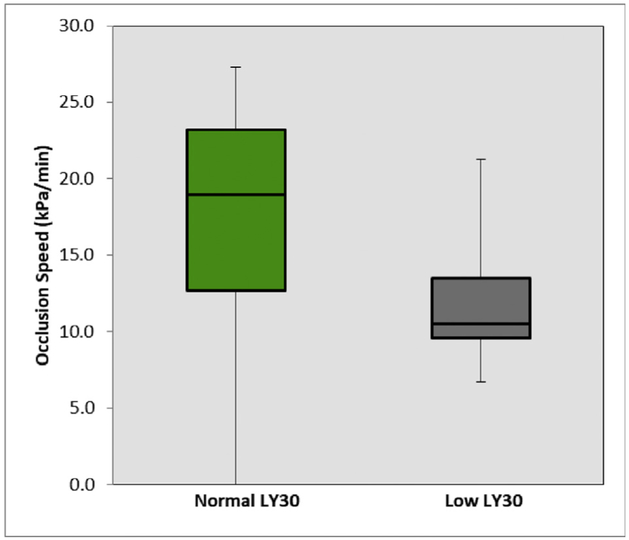
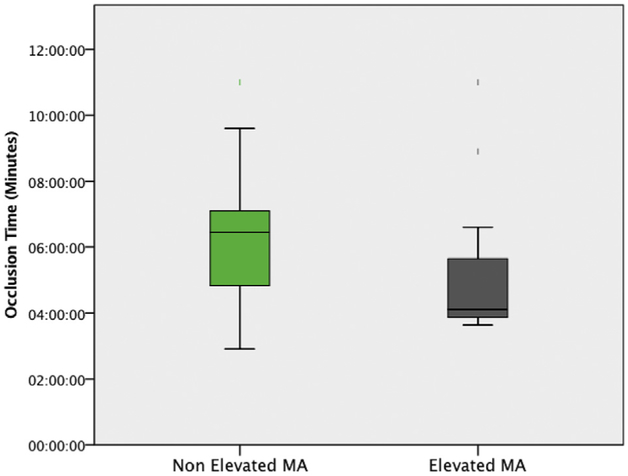
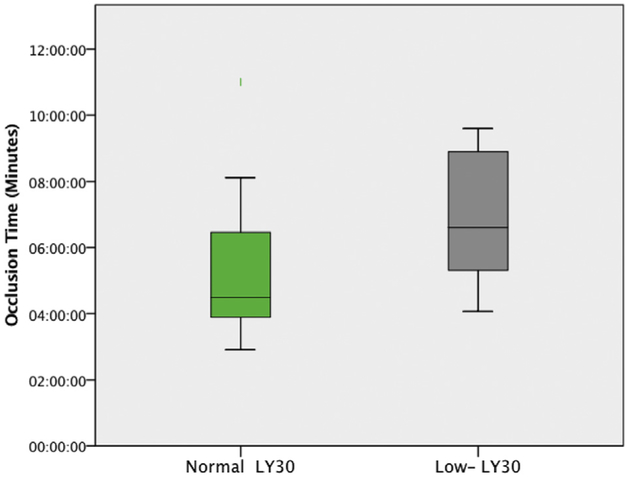
Thirty subjects were analyzed, including five controls. TEG-defined hypercoagulability by MA was detected in 52% of the inflammatory bowel disease/cancer patients; 0% was detected in the controls. There were no TEG measurements that significantly correlated with T-TAS AR and PL chip. However, in the presence of t-PA, T-TAS AR determined OSp to have an inverse relationship with TEG angle (-0.477, P = 0.012) and LY30 (-0.449, P = 0.019), and a positive correlation with R time (0.441 P = 0.021). In hypercoagulability determined by TEG MA, T-TAS PL had a significantly reduced OT (4:07 versus 6:27 min, P = 0.043). In hypercoagulability defined by TEG LY30, T-TAS PL had discordant findings, with a significantly prolonged OT (6:36 versus 4:30 min, P = 0.044) and a slower OSp (10.5 versus 19.0 kPa/min, P = 0.030).
Microfluidic coagulation assessment with T-TAS has an overall poor correlation with most TEG measurements in a predominantly hypercoagulable patient population, except in the presence of t-PA. The one anticipated finding was an elevated MA having a shorter time to platelet-mediated microfluidic occlusion, supporting the role of platelets and hypercoagulability. However, hypercoagulability defined by LY30 had opposing results in which a low LY30 was associated with a longer PL time to occlusion and slower OSp. These discordant findings warrant ongoing investigation into the relationship between clot strength and fibrinolysis under different flow conditions.
通过血栓弹力图(TEG)测量的凝血强度升高(最大振幅[MA])与血栓形成并发症相关。然而,由于该测量独立于时间、血流和血凝块降解,MA如何转化为血栓形成风险仍不清楚。我们假设在血流条件下,增加的凝血强度与凝血的时间依赖性测量以及对纤维蛋白溶解的抵抗力相关。
对有血栓形成并发症高风险的手术患者进行TEG和全血栓形成分析系统(T-TAS)分析。TEG高凝状态定义为r<10.2分钟、角度>59、MA>66或LY30<0.2%(基于健康对照数据,n=141)。T-TAS AR和PL芯片用于测量动脉剪切速率下的凝血情况。T-TAS测量包括闭塞开始时间、闭塞时间(OT)、闭塞速度(OSp)和总凝块生成(曲线下面积)。这些测量与TEG指标(R时间、角度、MA和LY30)相关。T-TAS和TEG检测均用组织型纤溶酶原激活剂(t-PA)进行挑战,以评估血凝块对纤维蛋白溶解的抵抗力。
分析了30名受试者,包括5名对照。在52%的炎症性肠病/癌症患者中检测到TEG定义的由MA导致的高凝状态;对照组中未检测到。没有TEG测量值与T-TAS AR和PL芯片显著相关。然而,在存在t-PA时,T-TAS AR确定OSp与TEG角度呈负相关(-0.477,P=0.012)和与LY30呈负相关(-0.449,P=0.019),与R时间呈正相关(0.441,P=0.021)。在由TEG MA确定的高凝状态下,T-TAS PL的OT显著缩短(4:07对6:27分钟,P=0.043)。在由TEG LY30定义的高凝状态下,T-TAS PL有不一致的结果,OT显著延长(6:36对4:30分钟,P=0.044)且OSp较慢(10.5对19.0 kPa/分钟,P=0.030)。
在主要为高凝状态的患者群体中,使用T-TAS进行的微流体凝血评估与大多数TEG测量的总体相关性较差,t-PA存在时除外。一个预期的发现是MA升高时血小板介导的微流体闭塞时间缩短,支持血小板和高凝状态的作用。然而,由LY30定义的高凝状态有相反的结果,即低LY30与PL闭塞时间延长和OSp较慢相关。这些不一致的发现需要对不同血流条件下凝血强度与纤维蛋白溶解之间的关系进行持续研究。