University of California San Diego, San Diego, CA, USA.
UC San Diego Health System, San Diego, CA, USA.
J Crohns Colitis. 2019 Feb 1;13(2):172-181. doi: 10.1093/ecco-jcc/jjy149.
This GEMINI 1 post hoc analysis evaluated vedolizumab efficacy for inducing deep remission in patients with ulcerative colitis and correlation between vedolizumab trough concentrations and deep remission rates.
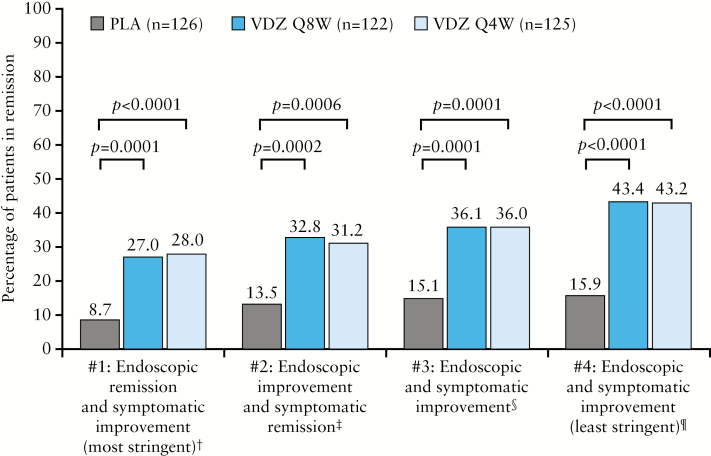
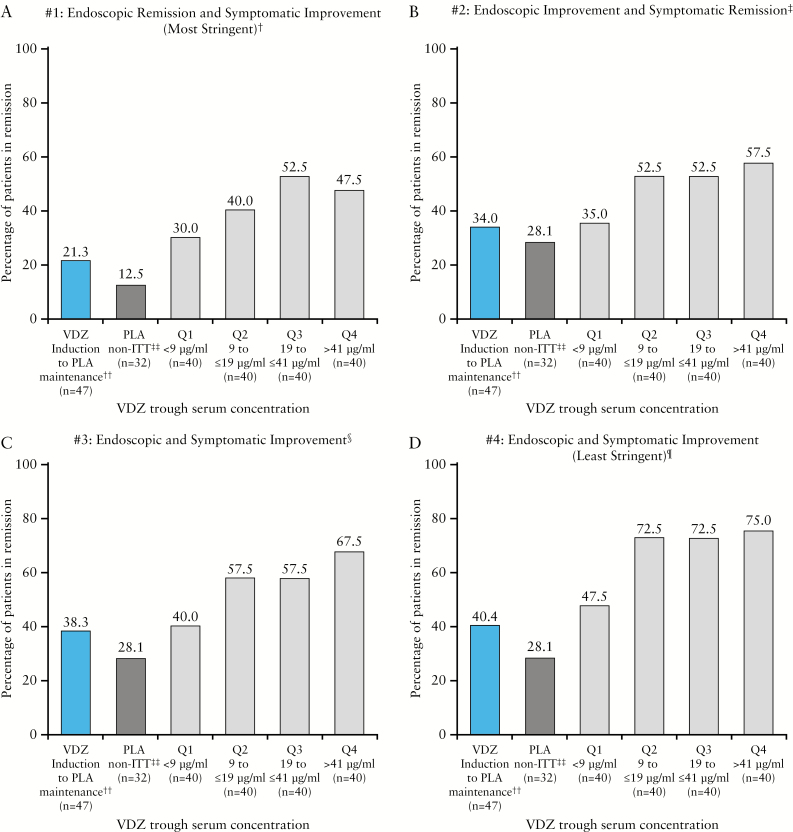
Week 6 vedolizumab responders were re-randomized to placebo or vedolizumab every 8 or 4 weeks. Deep remission at Week 52 was measured using four different definitions [from most to least stringent]: [1] Mayo Clinic endoscopic score = 0, rectal bleeding score = 0 and decrease or no change from baseline in stool frequency score; [2] endoscopic score ≤1, rectal bleeding score = 0 and stool frequency score = 0; [3] endoscopic score ≤1, rectal bleeding score = 0, decrease or no change from baseline stool frequency score, and total score [endoscopic score + rectal bleeding score + stool frequency score] ≤1; and [4] endoscopic score ≤1, rectal bleeding score = 0 and stool frequency score ≤1. Steady-state trough vedolizumab serum concentrations were evaluated.
At Week 6, 373 vedolizumab responders were re-randomized to maintenance placebo [n = 126] or vedolizumab every 8 [n = 122] or 4 [n = 125] weeks. Significantly more vedolizumab patients achieved deep remission at Week 52 for the most (placebo 8.7%, every 8 weeks 27.0% [p = 0.0001], every 4 weeks 28.0% [p < 0.0001]) and least (placebo 15.9%, every 8 weeks 43.4% [p < 0.0001], every 4 weeks 43.2% [p < 0.0001]) stringent definitions. Patients with higher vedolizumab trough concentration quartiles had higher deep remission rates [all definitions] compared with those with the lowest quartile or who received placebo.
Vedolizumab was associated with significantly higher deep remission rates than placebo at Week 52, regardless of deep remission definition [NCT00783718].
本 GEMINI 1 事后分析评估了维得利珠单抗诱导溃疡性结肠炎深度缓解的疗效,以及维得利珠单抗谷浓度与深度缓解率的相关性。
第 6 周维得利珠单抗应答者重新随机分为安慰剂或维得利珠单抗每 8 或 4 周 1 次。第 52 周采用 4 种不同定义(从最严格到最宽松)评估深度缓解:[1]Mayo 内镜评分=0,直肠出血评分=0,粪便频率评分较基线降低或不变;[2]内镜评分≤1,直肠出血评分=0,粪便频率评分=0;[3]内镜评分≤1,直肠出血评分=0,粪便频率评分较基线降低或不变,且总分[内镜评分+直肠出血评分+粪便频率评分]≤1;[4]内镜评分≤1,直肠出血评分=0,粪便频率评分≤1。评估稳态维得利珠单抗血清浓度。
第 6 周,373 例维得利珠单抗应答者重新随机分为维持治疗安慰剂组(n=126)、维得利珠单抗每 8 周组(n=122)和每 4 周组(n=125)。第 52 周时,更多的维得利珠单抗患者达到了最严格(安慰剂组 8.7%,每 8 周组 27.0%[p=0.0001],每 4 周组 28.0%[p<0.0001])和最宽松(安慰剂组 15.9%,每 8 周组 43.4%[p<0.0001],每 4 周组 43.2%[p<0.0001])定义的深度缓解。较高维得利珠单抗谷浓度四分位数的患者深度缓解率更高[所有定义],与最低四分位数或接受安慰剂的患者相比。
与安慰剂相比,无论深度缓解定义如何,第 52 周时维得利珠单抗与更高的深度缓解率相关[NCT00783718]。