Department of Neurosurgery, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Shuaifuyuan 1, Dong Cheng District, Beijing, 100730, China.
Sci Rep. 2018 Oct 4;8(1):14831. doi: 10.1038/s41598-018-33263-8.
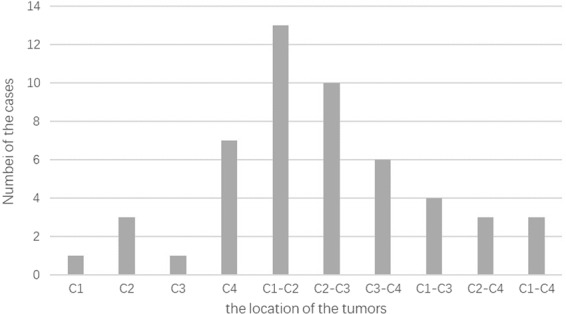
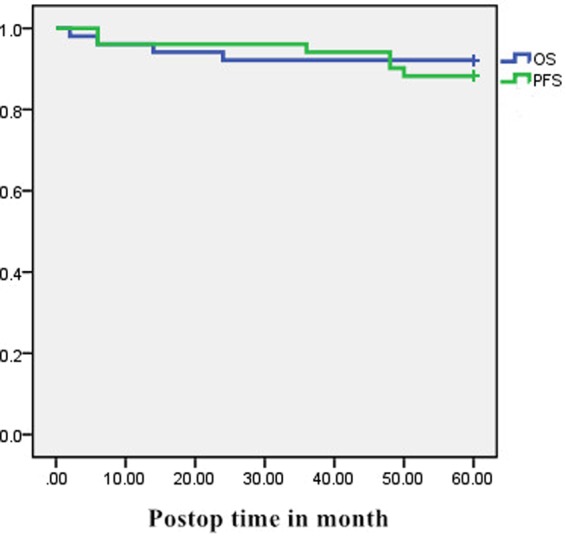
The literature discussing the long-term outcome after resection of upper cervical spinal cord tumors is limited. The purpose of this study was to review the progression-free survival (PFS), overall survival (OS), and long-term outcomes in a consecutive series of 51 patients with upper cervical spinal cord tumors who underwent surgery at our institution between 2005 and 2010. Patient outcome were evaluated using the Japanese Orthopaedic Association score (JOA) and the McCormick functional schema. Follow-up data was collected completely and the median follow-up time was 6.1 years. Gross total resection (GTR) was performed in 27 patients (52.94%) and subtotal resection (STR) in 24 patients (47.06%). Progression-free survival and overall survival at 5 years was 88.23% and 92.16%, respectively. Good prognosis was defined as 74.51% based on JOA scoring. The univariate analysis showed that patients over 60y, tumors located higher than C2, tumor size greater than 4 cm as well as malignant tumors and subtotal resection were factors indicating a poor prognosis. However, the multivariate regression analyses showed only the level of tumor and tumor size were independent risk factors for a poor prognosis. The gold standard treatment for intraspinal tumors is gross total resection and follow-up should be focused on patients with a high risk of poor prognosis.
有关上颈椎脊髓肿瘤切除术后长期结果的文献有限。本研究的目的是回顾 2005 年至 2010 年间在我们机构接受手术的 51 例上颈椎脊髓肿瘤患者的无进展生存率(PFS)、总生存率(OS)和长期结果。使用日本矫形协会评分(JOA)和 McCormick 功能图评估患者的预后。收集了完整的随访数据,中位随访时间为 6.1 年。27 例患者(52.94%)行全切除(GTR),24 例患者(47.06%)行次全切除(STR)。5 年无进展生存率和总生存率分别为 88.23%和 92.16%。根据 JOA 评分,预后良好定义为 74.51%。单因素分析显示,年龄>60 岁、肿瘤位于 C2 以上、肿瘤大小>4cm、肿瘤恶性和次全切除是预后不良的因素。然而,多因素回归分析显示,只有肿瘤水平和肿瘤大小是预后不良的独立危险因素。脊髓内肿瘤的金标准治疗是全切除,随访应重点关注预后不良风险较高的患者。