Gembruch Oliver, Chihi Mehdi, Haarmann Merle, Parlak Ahmet, Oppong Marvin Darkwah, Rauschenbach Laurèl, Michel Anna, Jabbarli Ramazan, Ahmadipour Yahya, Sure Ulrich, Dammann Philipp, Özkan Neriman
Department of Neurosurgery, University Hospital Essen, University of Duisburg-Essen, Hufelandstrasse 55, 45122 Essen, Germany.
Department of Neurosurgery, University Hospital Essen, University of Duisburg-Essen, Essen, Germany.
Ther Adv Neurol Disord. 2021 Nov 10;14:17562864211055694. doi: 10.1177/17562864211055694. eCollection 2021.
Spinal cord ependymomas account for 3-6% of all central nervous system tumors and around 60% of all intramedullary tumors. The aim of this study was to analyze the neurological outcome after surgery and to determine prognostic factors for functional outcome.
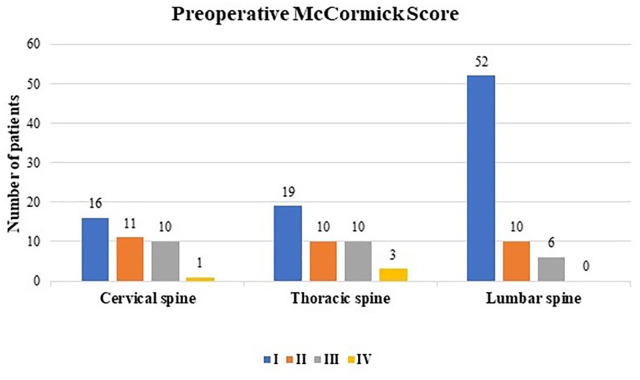
Patients treated surgically due to a spinal cord ependymoma between 1990 and 2018 were retrospectively included. Demographics, neurological symptoms, radiological parameters, histopathology, and neurological outcome (using McCormick Score [MCS]) were analyzed. Possible prognostic factors for neurological outcome were evaluated.
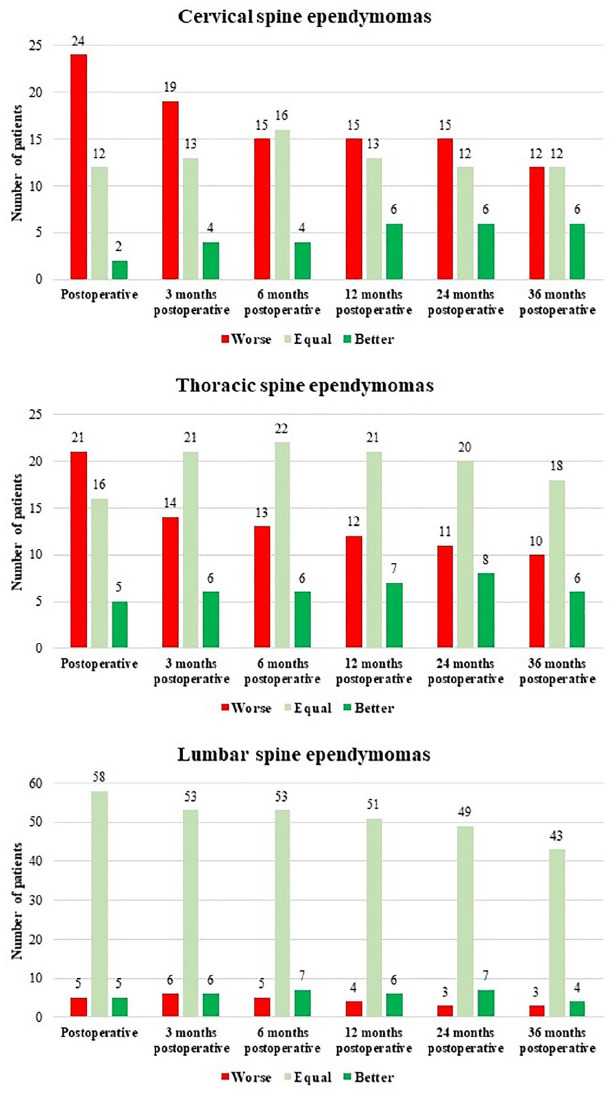
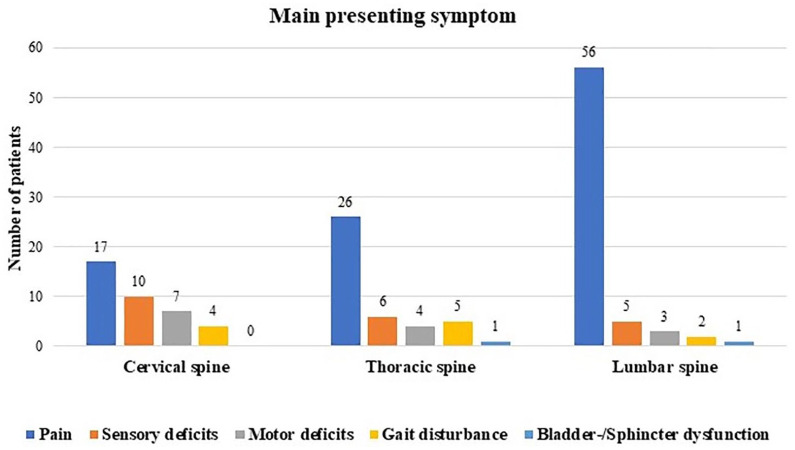
In total, 148 patients were included (76 males, 51.4%). The mean age was 46.7 ± 15.3 years. The median follow-up period was 6.8 ± 5.4 years. The prevalence was mostly in the lumbar spine (45.9%), followed by the thoracic spine (28.4%) and cervical spine (25.7%). Gross-total resection was achieved in 129 patients (87.2%). The recurrence rate was 8.1% and depended on the extent of tumor resection ( = 0.001). Postoperative temporary neurological deterioration was observed in 63.2% of patients with ependymomas of the cervical spine, 50.0% of patients with ependymomas of the thoracic spine, and 7.4% of patients with ependymomas of the lumbosacral region. MCS 1-2 was detected in nearly two-thirds of patients with cervical and thoracic spinal cord ependymoma 36 months after surgery. Neurological recovery was superior in thoracic spine ependymomas compared with cervical spine ependymomas. Poor preoperative functional condition (MCS >2), cervical and thoracic spine location, and tumor extension >2 vertebrae were independent predictors of poor neurological outcome.
Neurological deterioration was seen in the majority of cervical and thoracic spine ependymomas. Postoperative improvement was less in thoracic cervical spine ependymomas compared with thoracic spine ependymomas. Poor preoperative status and especially tumor extension >2 vertebrae are predictors of poor neurological outcome (MCS >2).
脊髓室管膜瘤占所有中枢神经系统肿瘤的3% - 6%,约占所有髓内肿瘤的60%。本研究旨在分析手术治疗后的神经学转归,并确定功能转归的预后因素。
回顾性纳入1990年至2018年间因脊髓室管膜瘤接受手术治疗的患者。分析人口统计学资料、神经症状、放射学参数、组织病理学及神经学转归(采用麦考密克评分[MCS])。评估神经学转归可能的预后因素。
共纳入148例患者(76例男性,占51.4%)。平均年龄为46.7 ± 15.3岁。中位随访期为6.8 ± 5.4年。病变部位多在腰椎(45.9%),其次为胸椎(28.4%)和颈椎(25.7%)。129例患者(87.2%)实现了肿瘤全切。复发率为8.1%,且取决于肿瘤切除范围(P = 0.001)。颈椎室管膜瘤患者中63.2%、胸椎室管膜瘤患者中50.0%以及腰骶部室管膜瘤患者中7.4%术后出现暂时性神经功能恶化。术后36个月,近三分之二的颈胸段脊髓室管膜瘤患者MCS为1 - 2级。与颈椎室管膜瘤相比,胸椎室管膜瘤的神经功能恢复更佳。术前功能状态差(MCS >2)、病变位于颈胸椎以及肿瘤累及超过2个椎体是神经学转归不良的独立预测因素。
大多数颈胸椎室管膜瘤患者出现神经功能恶化。与胸椎室管膜瘤相比,颈胸椎室管膜瘤术后改善较少。术前状态差,尤其是肿瘤累及超过2个椎体是神经学转归不良(MCS >2)的预测因素。