Department of Pharmaceutical Outcomes and Policy, College of Pharmacy, University of Florida, Gainesville, FL.
Department of Medicine, University of Florida, Gainesville, FL.
Hepatology. 2019 Mar;69(3):1032-1045. doi: 10.1002/hep.30303. Epub 2019 Feb 10.
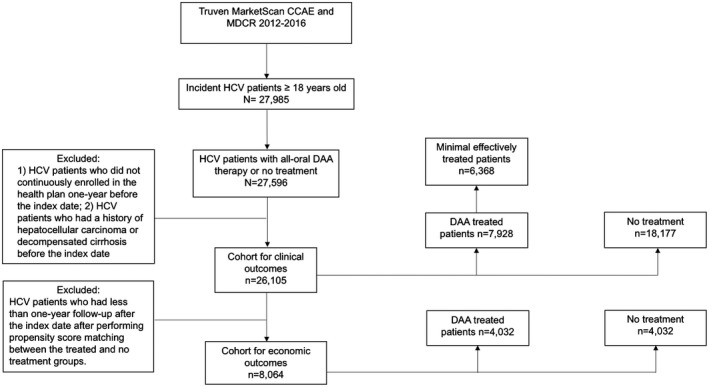
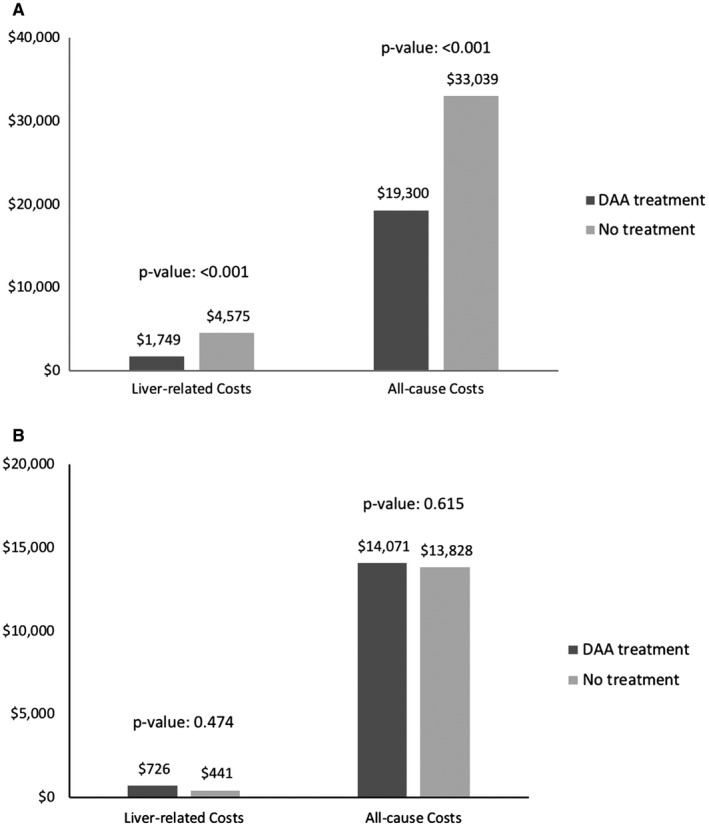
Approved treatment for hepatitis C virus (HCV) with all-oral direct-acting antivirals (DAA) therapy is now entering into its fourth year; however, little has been reported on the real-world clinical (decompensated cirrhosis [DCC] and hepatocellular carcinoma [HCC]) and economic outcomes. A retrospective cohort analysis of the Truven Health MarketScan Database (2012-2016) was conducted. In a cohort of 26,105 patients with newly diagnosed HCV, 30% received all-oral DAA therapy (DAA group) and 70% were not treated (untreated group). Multivariate Cox proportional hazards models were used to compare the risk of developing HCC and DCC, stratified by cirrhosis status. Among patients with cirrhosis (n = 2157), DAA therapy was associated with a 72% and a 62% lower incidence of HCC (hazard ratio [HR], 0.28; 95% confidence interval [CI], 0.15-0.52) and DCC (HR, 0.38; 95% CI, 0.26-0.56). Similarly, DAA therapy was associated with a 57% and a 58% lower incidence of HCC (HR, 0.43; 95% CI, 0.26-0.71) and DCC (HR, 0.42; 95% CI, 0.30-0.58) in patients with noncirrhotic HCV (n = 23,948). A propensity score-matched cohort of 8064 HCV-infected patients who had at least a 12-month follow-up after HCV treatment was included for economic analysis. For patients with cirrhosis in the DAA group, the mean adjusted liver-related costs ($1749 vs. $4575; P < 0.001) and all-cause medical costs ($19,300 vs. $33,039; P < 0.001) were significantly lower compared with those in the untreated group. The mean adjusted costs were not statistically different between the two groups among patients without cirrhosis. Conclusion: In the short term, all-oral DAA treatment for HCV infection was associated with a decreased risk of developing HCC and DCC, resulting in decreased health care costs, especially in patients with cirrhosis. A longitudinal study is necessary to confirm our findings.
目前,丙型肝炎病毒(HCV)的治疗已进入第四个年头,采用全口服直接作用抗病毒药物(DAA)治疗。然而,有关真实世界临床结局(失代偿性肝硬化[DCC]和肝细胞癌[HCC])和经济结局的报道甚少。本研究采用 Truven Health MarketScan 数据库(2012-2016 年)进行回顾性队列分析。在 26105 例新诊断 HCV 患者中,30%接受了全口服 DAA 治疗(DAA 组),70%未接受治疗(未治疗组)。采用多变量 Cox 比例风险模型,按肝硬化状态对 HCC 和 DCC 发生风险进行分层比较。在 2157 例肝硬化患者中,DAA 治疗 HCC 的发生率降低 72%,DCC 的发生率降低 62%(风险比[HR],0.28;95%置信区间[CI],0.15-0.52)。同样,在无肝硬化的 HCV 患者(n=23948)中,DAA 治疗 HCC 的发生率降低 57%,DCC 的发生率降低 58%(HR,0.43;95%CI,0.26-0.71)和 DCC(HR,0.42;95%CI,0.30-0.58)。纳入了一项 HCV 感染患者的倾向性评分匹配队列(n=8064),这些患者在 HCV 治疗后至少有 12 个月的随访,用于进行经济分析。在 DAA 组的肝硬化患者中,与未治疗组相比,肝相关费用($1749 比$4575;P < 0.001)和全因医疗费用($19300 比$33039;P < 0.001)显著降低。在无肝硬化患者中,两组之间的平均调整成本无统计学差异。结论:短期内,丙型肝炎病毒感染的全口服 DAA 治疗与 HCC 和 DCC 风险降低相关,从而降低医疗保健费用,尤其是在肝硬化患者中。需要进行纵向研究来证实我们的研究结果。