Piccoli Giorgina Barbara, Nielsen Louise, Gendrot Lurilyn, Fois Antioco, Cataldo Emanuela, Cabiddu Gianfranca
Néphrologie Centre Hospitalier Le Mans, Avenue Roubillard 196, 72000 Le Mans, France.
Dipartimento di Scienze Cliniche e Biologiche, University of Torino, Ospedale san Luigi, Regione Gonzole, 10100 Torino, Italy.
J Clin Med. 2018 Oct 8;7(10):331. doi: 10.3390/jcm7100331.
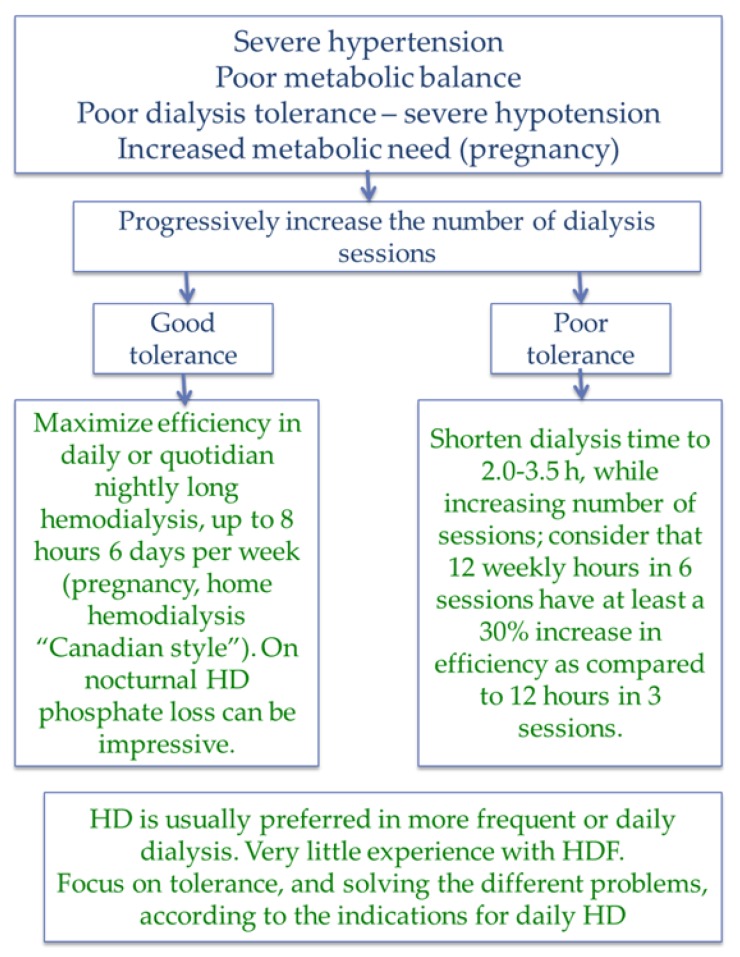
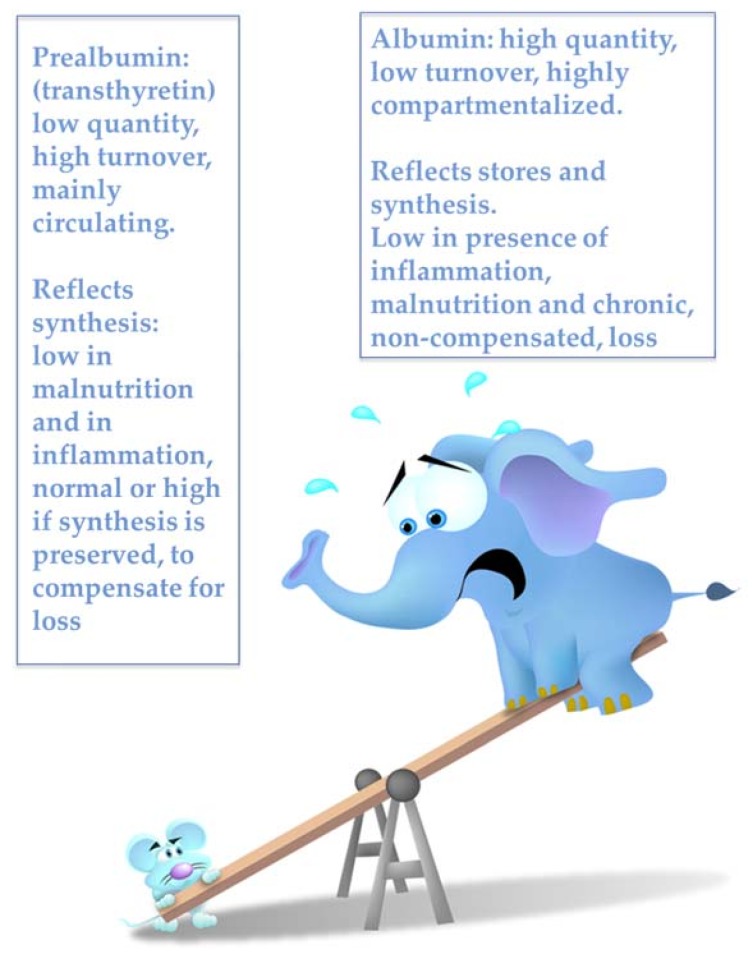
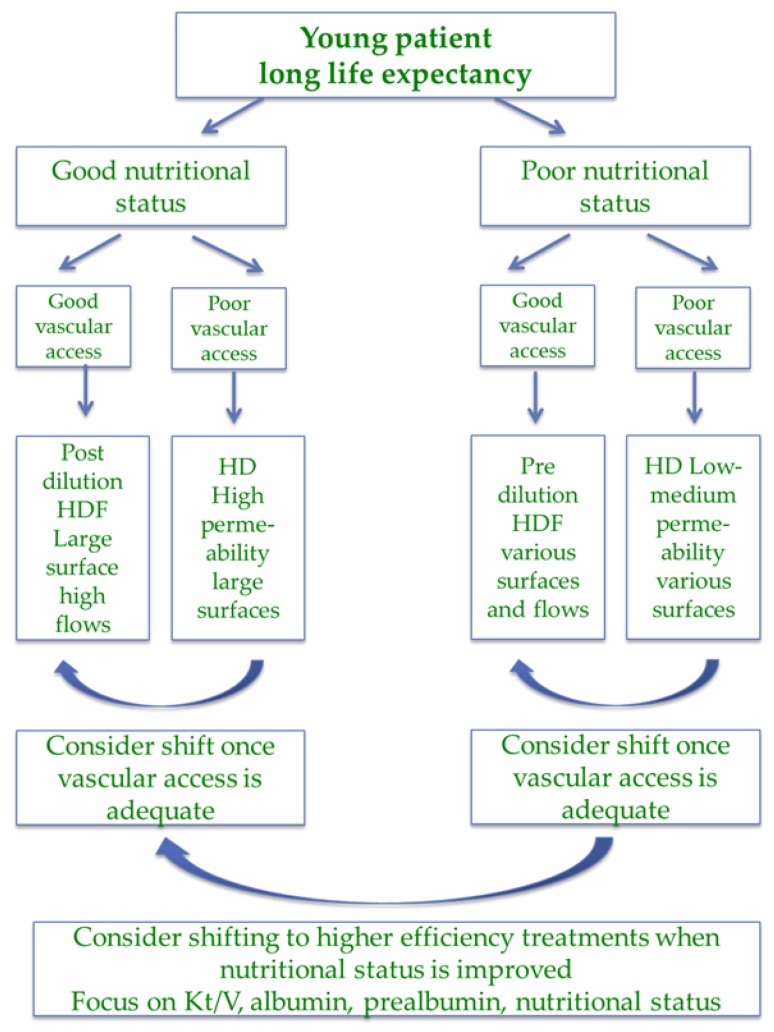
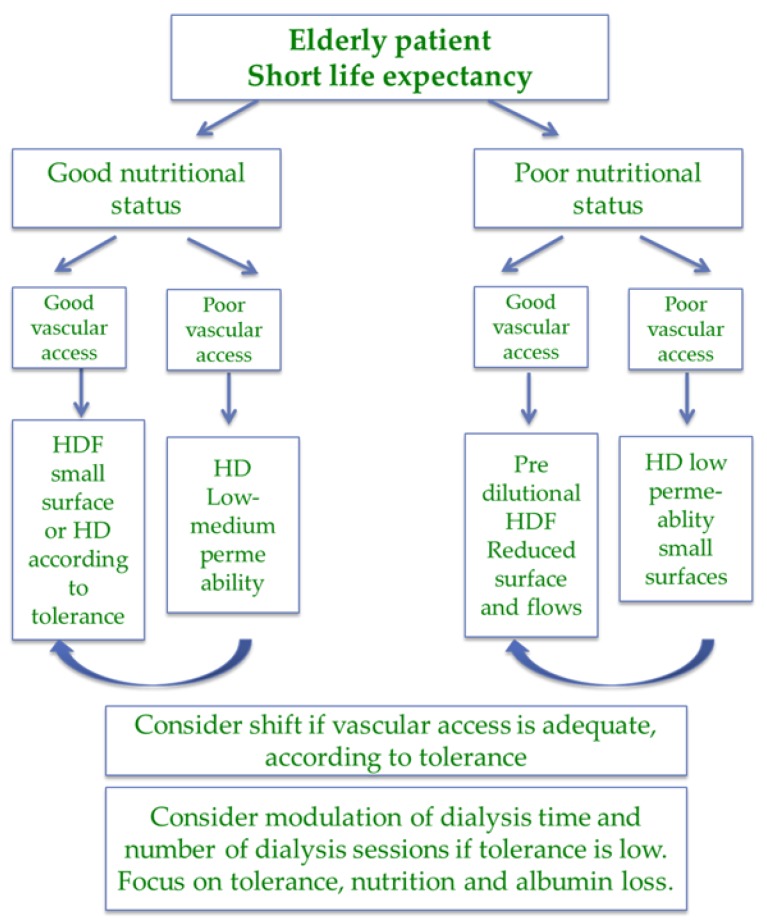
There is no simple way to prescribe hemodialysis. Changes in the dialysis population, improvements in dialysis techniques, and different attitudes towards the initiation of dialysis have influenced treatment goals and, consequently, dialysis prescription. However, in clinical practice prescription of dialysis still often follows a "one size fits all" rule, and there is no agreed distinction between treatment goals for the younger, lower-risk population, and for older, high comorbidity patients. In the younger dialysis population, efficiency is our main goal, as assessed by the demonstrated close relationship between depuration (tested by kinetic adequacy) and survival. In the ageing dialysis population, tolerance is probably a better objective: "good dialysis" should allow the patient to attain a stable metabolic balance with minimal dialysis-related morbidity. We would like therefore to open the discussion on a personalized approach to dialysis prescription, focused on efficiency in younger patients and on tolerance in older ones, based on life expectancy, comorbidity, residual kidney function, and nutritional status, with particular attention placed on elderly, high-comorbidity populations, such as the ones presently treated in most European centers. Prescription of dialysis includes reaching decisions on the following elements: dialysis modality (hemodialysis (HD) or hemodiafiltration (HDF)); type of membrane (permeability, surface); and the frequency and duration of sessions. Blood and dialysate flow, anticoagulation, and reinfusion (in HDF) are also briefly discussed. The approach described in this concept paper was developed considering the following items: nutritional markers and integrated scores (albumin, pre-albumin, cholesterol; body size, Body Mass Index (BMI), Malnutrition Inflammation Score (MIS), and Subjective Global Assessment (SGA)); life expectancy (age, comorbidity (Charlson Index), and dialysis vintage); kinetic goals (Kt/V, normalized protein catabolic rate (n-PCR), calcium phosphate, parathyroid hormone (PTH), beta-2 microglobulin); technical aspects including vascular access (fistula versus catheter, degree of functionality); residual kidney function and weight gain; and dialysis tolerance (intradialytic hypotension, post-dialysis fatigue, and subjective evaluation of the effect of dialysis on quality of life). In the era of personalized medicine, we hope the approach described in this concept paper, which requires validation but has the merit of providing innovation, may be a first step towards raising attention on this issue and will be of help in guiding dialysis choices that exploit the extraordinary potential of the present dialysis "menu".
目前还没有简单的方法来规定血液透析方案。透析人群的变化、透析技术的改进以及对开始透析的不同态度都影响了治疗目标,进而影响了透析方案的制定。然而,在临床实践中,透析方案的制定往往仍遵循“一刀切”的规则,对于年轻、低风险人群和老年、高合并症患者的治疗目标,并没有达成共识。在年轻的透析人群中,效率是我们的主要目标,这一点可通过已证实的清除率(通过动力学充分性测试)与生存率之间的密切关系来评估。在老龄化的透析人群中,耐受性可能是一个更好的目标:“良好的透析”应使患者在透析相关发病率最小的情况下达到稳定的代谢平衡。因此,我们希望开启关于个性化透析方案制定方法的讨论,该方法基于预期寿命、合并症、残余肾功能和营养状况,关注年轻患者的效率和老年患者的耐受性,尤其关注老年、高合并症人群,比如目前大多数欧洲中心所治疗的这类患者。透析方案的制定包括就以下要素做出决策:透析方式(血液透析(HD)或血液透析滤过(HDF));膜的类型(通透性、表面积);以及治疗次数和时长。还简要讨论了血流量和透析液流量、抗凝以及(血液透析滤过中的)再输注。本概念文件中描述的方法是在考虑以下各项的基础上制定的:营养指标和综合评分(白蛋白、前白蛋白、胆固醇;体型、体重指数(BMI)、营养不良炎症评分(MIS)和主观全面评定(SGA));预期寿命(年龄、合并症(查尔森指数)和透析龄);动力学目标(Kt/V、标准化蛋白分解代谢率(n-PCR)、钙磷、甲状旁腺激素(PTH)、β2微球蛋白);技术方面,包括血管通路(动静脉内瘘与导管,功能程度);残余肾功能和体重增加;以及透析耐受性(透析中低血压、透析后疲劳,以及透析对生活质量影响的主观评估)。在个性化医疗时代,我们希望本概念文件中描述的方法(该方法需要验证,但具有提供创新的优点)可能是提高对该问题关注度的第一步,并将有助于指导透析选择,充分利用当前透析“菜单”的非凡潜力。