Barros-Gomes Sergio, El Sabbagh Abdallah, Eleid Mackram F, Mankrad Sunil V
Division of Cardiovascular Diseases, Mayo Clinic, Rochester, Minnesota, USA
Echo Res Pract. 2018 Dec 1;5(4):I9-I10. doi: 10.1530/ERP-18-0044.
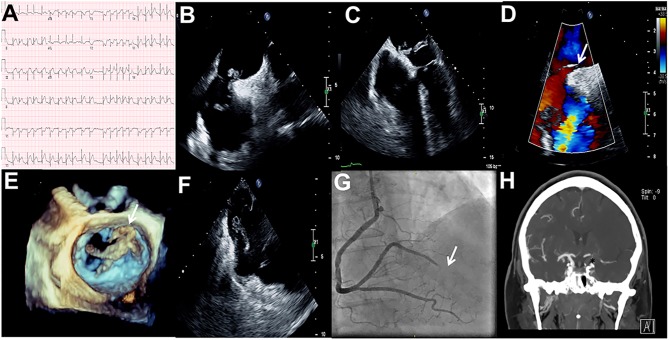
Non-atherosclerotic myocardial infarction (MI) is an important but often misdiagnosed cause of acute MI. Furthermore, non-atherosclerotic MI with concomitant acute stroke and pulmonary embolism due to in-transit thrombus across a patent foramen ovale (PFO) is a rare but potentially fatal combination (1, 2, 3). Early detection of this clinical entity can facilitate delivery of targeted therapies and avoid poor outcome (1, 2). Here, we describe a 68-year-old female with hypertension, tobacco abuse and chronic obstructive pulmonary disease presenting with facial droop, right arm weakness and aphasia. Head computed tomography (CT) without contrast was unremarkable. ECG showed an acute inferolateral ST-elevation MI (Fig. 1, Panel A). As patient presented with both an acute neurological deficit and MI, clinical suspicion of non-atherosclerotic MI was raised and the patient underwent concurrent emergency coronary angiography (CAG) and transesophageal echocardiogram (TEE). TEE revealed highly mobile masses in the left and right atrium (Fig. 1, Panel B and Video 1). The large mass (thrombus or cast of a deep venous thrombus) was caught in a PFO (Fig. 1, Panel C, D, E and Videos 2, 3). A second smaller mass/thrombus was seen on the Eustachian valve near the right atrial/inferior vena cava junction (Fig. 1, Panel F and Video 4). CAG confirmed a 100% occluded distal right posterolateral artery suggestive of an embolic phenomenon. The patient underwent successful thrombectomy, retrieving a large thrombus burden (Fig. 1, Panel G and Videos 5, 6, 7). CT angiography showed occluded internal carotid artery (Fig. 1, Panel H). Pathology from thrombectomy confirmed fibrin-rich thrombus. The patient had bilateral lower extremity deep vein thrombosis and bilateral diffuse pulmonary embolisms.
非动脉粥样硬化性心肌梗死(MI)是急性心肌梗死的一个重要但常被误诊的病因。此外,因卵圆孔未闭(PFO)处移行血栓导致的非动脉粥样硬化性心肌梗死合并急性脑卒中及肺栓塞是一种罕见但可能致命的组合(1, 2, 3)。早期发现这一临床实体有助于实施针对性治疗并避免不良预后(1, 2)。在此,我们描述一名68岁女性,有高血压、吸烟史和慢性阻塞性肺疾病,出现面部下垂、右臂无力和失语。头颅非增强计算机断层扫描(CT)未见异常。心电图显示急性下侧壁ST段抬高型心肌梗死(图1,A组)。由于患者同时出现急性神经功能缺损和心肌梗死,临床怀疑为非动脉粥样硬化性心肌梗死,遂对患者同时进行了急诊冠状动脉造影(CAG)和经食管超声心动图(TEE)检查。TEE显示左、右心房内有高度活动的团块(图1,B组及视频1)。一个大的团块(血栓或深部静脉血栓的栓子)卡在卵圆孔未闭处(图1,C、D、E组及视频2、3)。在右心房/下腔静脉交界处的欧氏瓣附近可见第二个较小的团块/血栓(图1,F组及视频4)。CAG证实右后外侧动脉远端100%闭塞,提示栓塞现象。患者成功进行了血栓切除术,取出了大量血栓负荷(图1,G组及视频5、6、7)。CT血管造影显示颈内动脉闭塞(图1,H组)。血栓切除术的病理结果证实为富含纤维蛋白的血栓。患者双侧下肢深静脉血栓形成及双侧弥漫性肺栓塞。