Department of Epidemiology of Microbial Diseases, Yale School of Public Health, New Haven, Connecticut.
Center for Health Economics Research and Modeling of Infectious Diseases, University of Antwerp, Belgium.
J Infect Dis. 2018 Nov 10;218(suppl_4):S255-S267. doi: 10.1093/infdis/jiy471.
Blood culture is the standard diagnostic method for typhoid and paratyphoid (enteric) fever in surveillance studies and clinical trials, but sensitivity is widely acknowledged to be suboptimal. We conducted a systematic review and meta-analysis to examine sources of heterogeneity across studies and quantified the effect of blood volume.
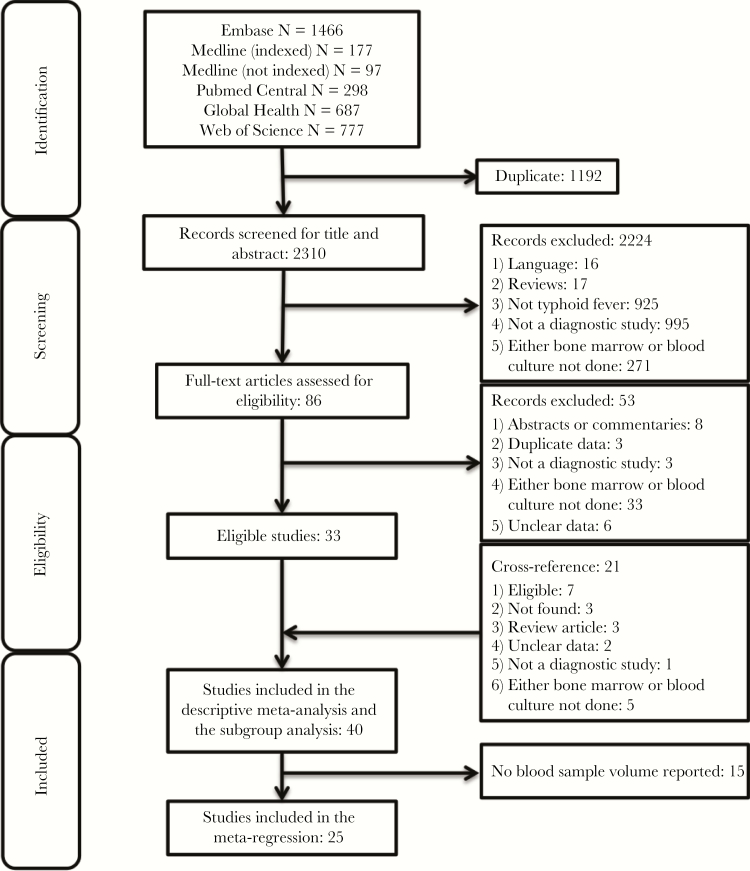
We searched the literature to identify all studies that performed blood culture alongside bone marrow culture (a gold standard) to detect cases of enteric fever. We performed a meta-regression analysis to quantify the relationship between blood sample volume and diagnostic sensitivity. Furthermore, we evaluated the impact of patient age, antimicrobial use, and symptom duration on sensitivity.
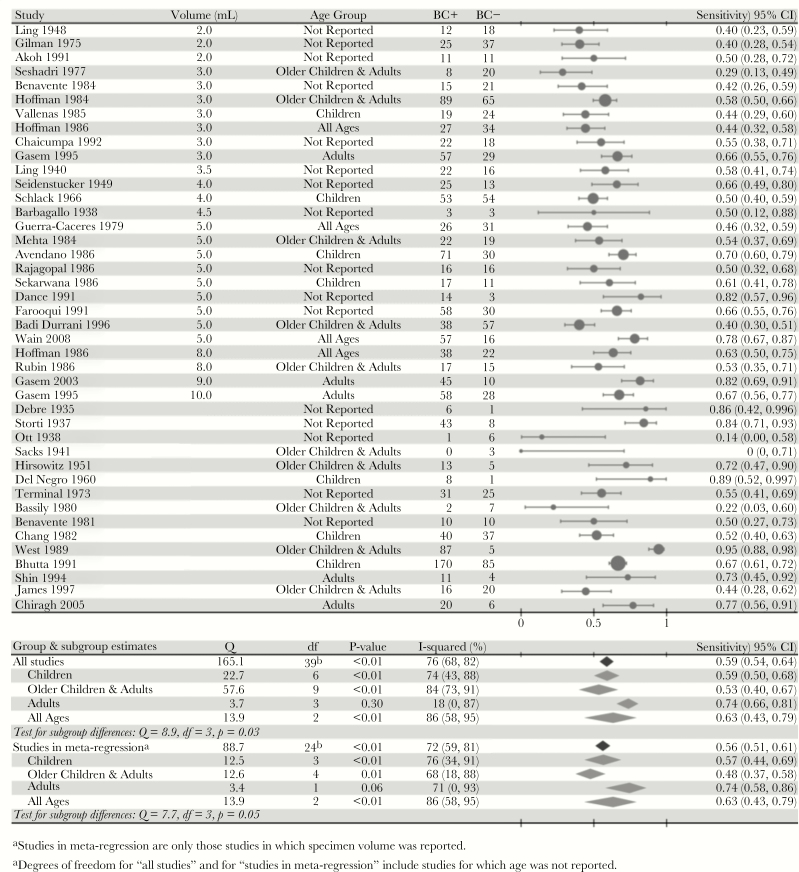
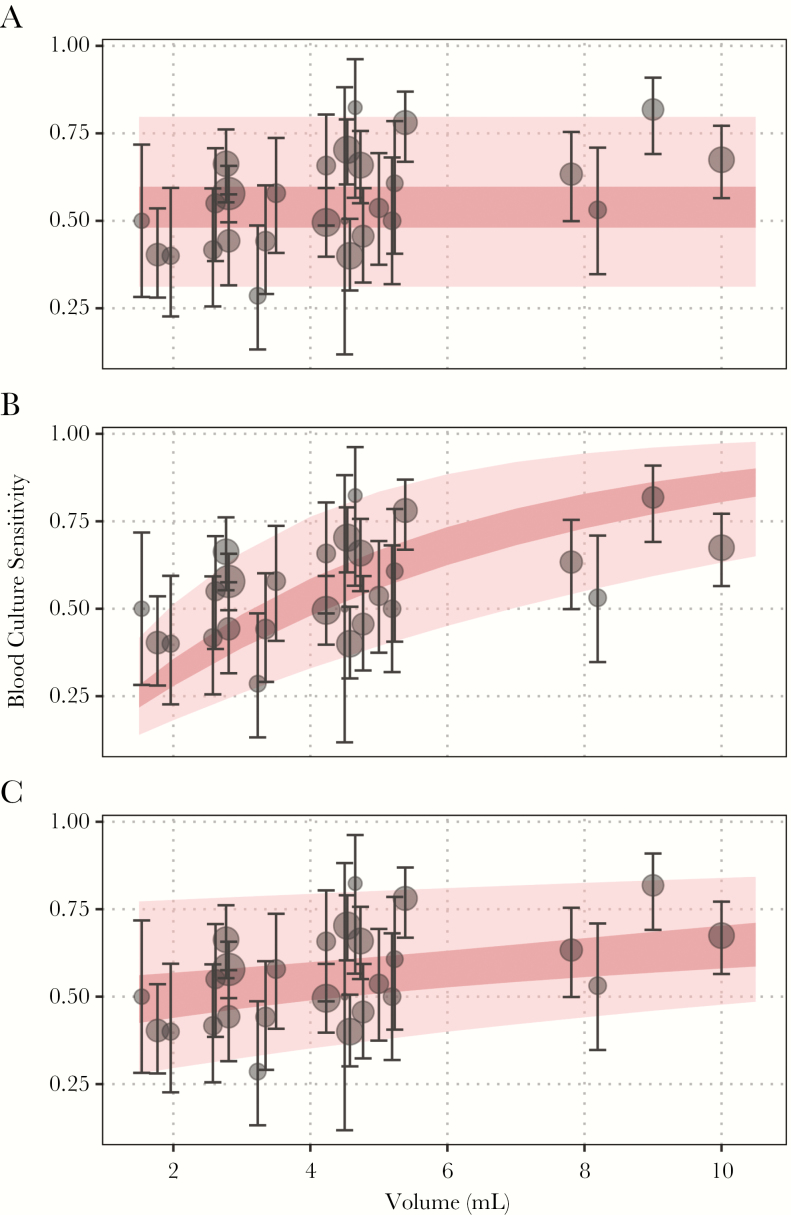
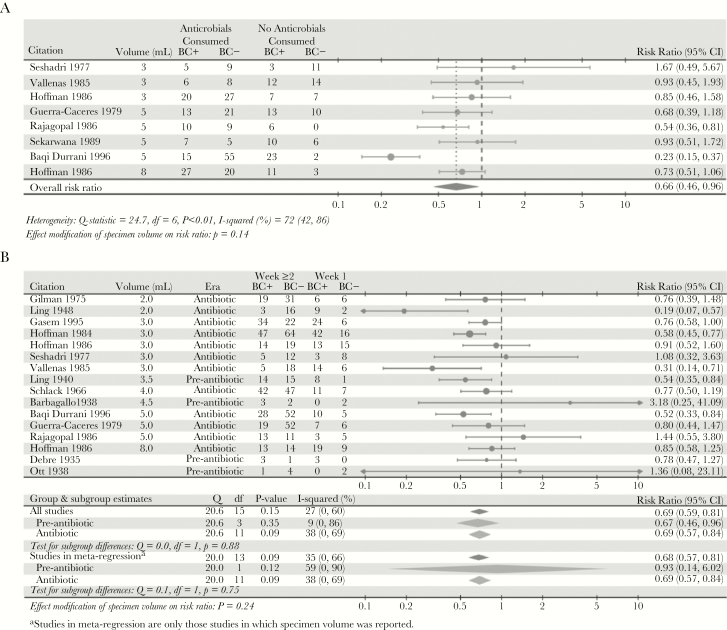
We estimated blood culture diagnostic sensitivity was 0.59 (95% confidence interval [CI], 0.54-0.64) with significant between-study heterogeneity (I2, 76% [95% CI, 68%-82%]; P < .01). Sensitivity ranged from 0.51 (95% CI, 0.44-0.57) for a 2-mL blood specimen to 0.65 (95% CI, 0.58-0.70) for a 10-mL blood specimen, indicative of a relationship between specimen volume and sensitivity. Subgroup analysis showed significant heterogeneity by patient age and a weak trend towards higher sensitivity among more recent studies. Sensitivity was 34% lower (95% CI, 4%-54%) among patients with prior antimicrobial use and 31% lower after the first week of symptoms (95% CI, 19%-41%). There was no evidence of confounding by patient age, antimicrobial use, symptom duration, or study date on the relationship between specimen volume and sensitivity.
The relationship between the blood sample volume and culture sensitivity should be accounted for in incidence and next-generation diagnostic studies.
血培养是监测研究和临床试验中伤寒和副伤寒(肠热)的标准诊断方法,但灵敏度被广泛认为不高。我们进行了系统评价和荟萃分析,以检查研究之间异质性的来源,并量化了血容量的影响。
我们搜索了文献,以确定所有进行血液培养与骨髓培养(金标准)相结合以检测肠热病病例的研究。我们进行了荟萃回归分析,以量化血样量与诊断灵敏度之间的关系。此外,我们评估了患者年龄、抗菌药物使用和症状持续时间对灵敏度的影响。
我们估计血培养诊断灵敏度为 0.59(95%置信区间 [CI],0.54-0.64),存在显著的研究间异质性(I2,76% [95% CI,68%-82%];P <.01)。灵敏度范围从 2 毫升血样的 0.51(95% CI,0.44-0.57)到 10 毫升血样的 0.65(95% CI,0.58-0.70),表明标本量与灵敏度之间存在关系。亚组分析显示,患者年龄存在显著异质性,近期研究显示灵敏度呈上升趋势。在有既往抗菌药物使用的患者中,灵敏度降低了 34%(95% CI,4%-54%),在症状出现第一周后,灵敏度降低了 31%(95% CI,19%-41%)。在血样量与灵敏度之间的关系上,没有证据表明患者年龄、抗菌药物使用、症状持续时间或研究日期存在混杂。
在发病率和下一代诊断研究中,应考虑血样量与培养灵敏度之间的关系。