Sex Transm Dis. 2019 Feb;46(2):91-97. doi: 10.1097/OLQ.0000000000000914.
Sub-optimal cervical cancer screening in low- and middle-income countries contributes to preventable cervical cancer deaths, particularly among human immunodeficiency virus (HIV)-positive women. We assessed feasibility and outcomes of integrating cervical cancer screening into safer conception services for HIV-affected women.
At a safer conception service in Johannesburg, South Africa, HIV-affected women desiring pregnancy received a standard package of care designed to minimize HIV transmission risks while optimizing prepregnancy health. All eligible women were offered Papanicolaou smear, and those with significant pathology were referred for colposcopy before attempting pregnancy. Multivariable analyses identified associations between patient characteristics and abnormal pathology.
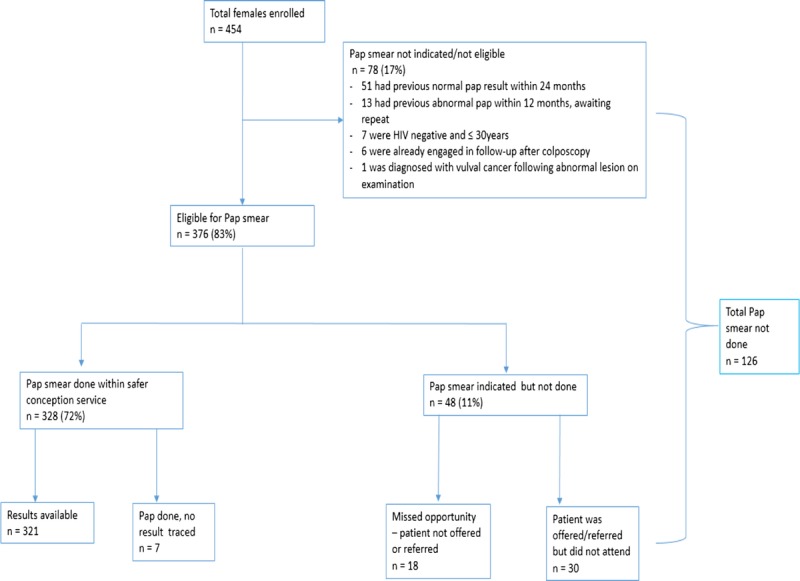
In total, 454 women were enrolled between June 2015 and April 2017. At enrolment, 91% were HIV-positive, 92% were on antiretroviral therapy (ART) and 82% virally suppressed. Eighty-three percent (376 of 454) of clients were eligible for cervical cancer screening and 85% (321 of 376) of these completed screening. More than half had abnormal cervical pathology (185 of 321) and 20% required colposcopy for possible high-grade or persistently atypical lesions (64 of 321). Compared with HIV-negative women, abnormal pathology was more likely among HIV-positive women, both those on ART <2 years (adjusted prevalence ratio, 2.5; 95% confidence interval, 1.2-5.0) and those on ART 2 years or longer (adjusted prevalence ratio, 2.1; 95% confidence interval, 1.0-4.2).
Integrating cervical cancer screening into safer conception care was feasible with high coverage, including for HIV-positive women. Significant pathology, requiring colposcopy, was common, even among healthy women on ART. Safer conception services present an opportunity for integration of cervical cancer screening to avert preventable cancer-related deaths among HIV-affected women planning pregnancy.
中低收入国家宫颈癌筛查不理想,导致可预防的宫颈癌死亡,尤其是在艾滋病毒(HIV)阳性妇女中。我们评估了将宫颈癌筛查纳入受 HIV 影响的妇女安全受孕服务中的可行性和结果。
在南非约翰内斯堡的一项安全受孕服务中,希望怀孕的受 HIV 影响的妇女接受了一套标准的护理方案,旨在最大限度地降低 HIV 传播风险,同时优化孕前健康。所有符合条件的妇女都接受巴氏涂片检查,对有明显病理学表现的妇女在尝试怀孕前进行阴道镜检查。多变量分析确定了患者特征与异常病理学之间的关联。
共有 454 名妇女于 2015 年 6 月至 2017 年 4 月期间入组。入组时,91%为 HIV 阳性,92%正在接受抗逆转录病毒治疗(ART),82%病毒得到抑制。83%(454 名患者中的 376 名)符合宫颈癌筛查条件,85%(376 名患者中的 321 名)完成了筛查。超过一半的人有异常宫颈病理学(321 名患者中的 185 名),20%(321 名患者中的 64 名)需要阴道镜检查以排除高级别或持续性非典型病变的可能性。与 HIV 阴性妇女相比,HIV 阳性妇女,包括接受 ART 治疗不足 2 年(调整后患病率比,2.5;95%置信区间,1.2-5.0)和接受 ART 治疗 2 年或更长时间(调整后患病率比,2.1;95%置信区间,1.0-4.2)的妇女,异常病理学更常见。
将宫颈癌筛查纳入安全受孕护理是可行的,覆盖率高,包括 HIV 阳性妇女。即使在接受 ART 治疗的健康妇女中,也存在需要阴道镜检查的大量病理学表现,这是常见的。安全受孕服务提供了将宫颈癌筛查纳入其中的机会,以避免计划怀孕的受 HIV 影响的妇女发生可预防的癌症相关死亡。