Mwenda Valerian, Murage David, Kilonzo Catherine, Bor Joan-Paula, Njiri Patricia, Osiro Lance, Nyangasi Mary, Arbyn Marc, Tummers Philippe, Temmerman Marleen
National Cancer Control Program, Ministry of Health, Nairobi, Kenya.
Field Epidemiology and Laboratory Program, Ministry of Health, Nairobi, Kenya.
Front Oncol. 2024 Jul 2;14:1371529. doi: 10.3389/fonc.2024.1371529. eCollection 2024.
Cervical cancer is the leading cause of cancer deaths among women in Kenya. In the context of the Global strategy to accelerate the elimination of cervical cancer as a public health problem, Kenya is currently implementing screening and treatment scale-up. For effectively tracking the scale-up, a baseline assessment of cervical cancer screening and treatment service availability and readiness was conducted in 25 priority counties. We describe the findings of this assessment in the context of elimination efforts in Kenya.
The survey was conducted from February 2021 to January 2022. All public hospitals in the target counties were included. We utilized healthcare workers trained in preparation for the scale-up as data collectors in each sub-county. Two electronic survey questionnaires (screening and treatment; and laboratory components) were used for data collection. All the health system building blocks were assessed. We used descriptive statistics to summarize the main service readiness indicators.
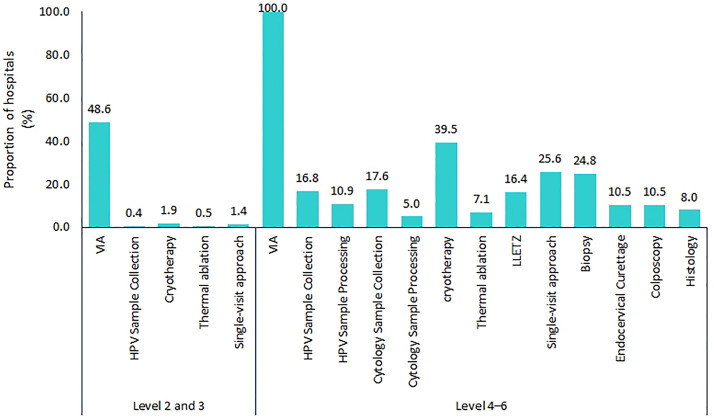
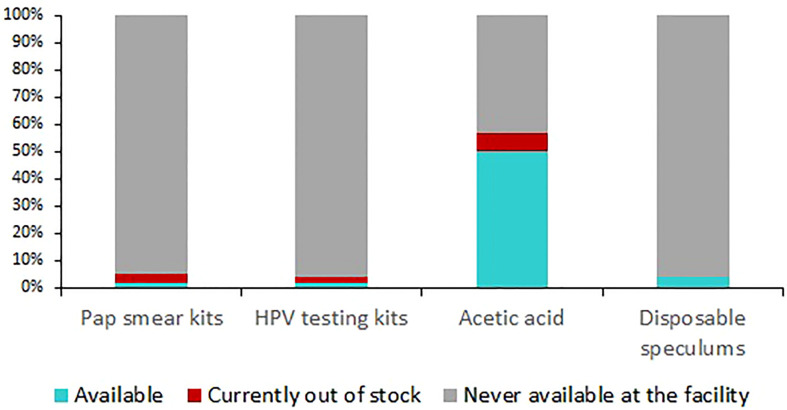
Of 3,150 hospitals surveyed, 47.6% (1,499) offered cervical cancer screening only, while 5.3% (166) offered both screening and treatment for precancer lesions. Visual inspection with acetic acid (VIA) was used in 96.0% (1,599/1,665) of the hospitals as primary screening modality and HPV testing was available in 31 (1.0%) hospitals. Among the 166 hospitals offering treatment for precancerous lesions, 79.5% (132/166) used cryotherapy, 18.7% (31/166) performed thermal ablation and 25.3% (42/166) performed large loop excision of the transformation zone (LLETZ). Pathology services were offered in only 7.1% (17/238) of the hospitals expected to have the service (level 4 and above). Only 10.8% (2,955/27,363) of healthcare workers were trained in cervical cancer screening and treatment; of these, 71.0% (2,097/2,955) were offering the services. Less than half of the hospitals had cervical cancer screening and treatment commodities at time of survey. The main health system strength was presence of multiple screening points at hospitals, but frequent commodity stock-outs was a key weakness.
Training, commodities, and diagnostic services are major gaps in the cervical cancer program in Kenya. To meet the 2030 elimination targets, the national and county governments should ensure adequate financing, training, and service integration, especially at primary care level.
宫颈癌是肯尼亚女性癌症死亡的主要原因。在加速消除作为公共卫生问题的宫颈癌的全球战略背景下,肯尼亚目前正在扩大筛查和治疗规模。为有效跟踪扩大规模的情况,在25个重点县对宫颈癌筛查和治疗服务的可及性及准备情况进行了基线评估。我们在肯尼亚的消除努力背景下描述了该评估的结果。
调查于2021年2月至2022年1月进行。纳入了目标县的所有公立医院。我们利用为扩大规模培训的医护人员作为每个次县的数据收集员。使用两份电子调查问卷(筛查和治疗;以及实验室部分)进行数据收集。对所有卫生系统组成部分进行了评估。我们使用描述性统计来总结主要的服务准备指标。
在接受调查的3150家医院中,47.6%(1499家)仅提供宫颈癌筛查,而5.3%(166家)同时提供癌前病变的筛查和治疗。96.0%(1599/1665)的医院使用醋酸目视检查(VIA)作为主要筛查方式,31家(1.0%)医院可进行HPV检测。在166家提供癌前病变治疗的医院中,79.5%(132/166)使用冷冻疗法,18.7%(31/166)进行热消融,25.3%(42/166)进行转化区大环形切除术(LLETZ)。预计应提供病理服务的医院中只有7.1%(17/238)提供了该服务(4级及以上医院)。只有10.8%(2955/27363)的医护人员接受了宫颈癌筛查和治疗培训;其中,71.0%(2097/2955)提供这些服务。调查时不到一半的医院有宫颈癌筛查和治疗用品。卫生系统的主要优势是医院有多个筛查点,但经常出现用品缺货是一个关键弱点。
培训、用品和诊断服务是肯尼亚宫颈癌项目的主要差距。为实现2030年消除目标,国家和县政府应确保充足的资金、培训和服务整合,尤其是在初级保健层面。