Ballester Leonor, Martínez Rafael, Méndez Juan, Miró Gloria, Solsona Manel, Palomera Elisabeth, Capdevila Josep Anton, Rodriguez Alejandro, Yébenes Juan Carlos
Servei de Medicina Interna, Hospital de Mataró, Mataró, 08304 Barcelona, Spain.
Servei de Medicina Intensiva, Hospital de Mataró, Mataró, 08304 Barcelona, Spain.
Med Sci (Basel). 2018 Oct 10;6(4):91. doi: 10.3390/medsci6040091.
Sepsis diagnosis can be incorrectly associated with the presence of hypotension during an infection, so the detection and management of non-hypotensive sepsis can be delayed. We aimed to evaluate how the presence or absence of hypotension, on admission at the emergency department, affects the initial management and outcomes of patients with community-onset severe sepsis.
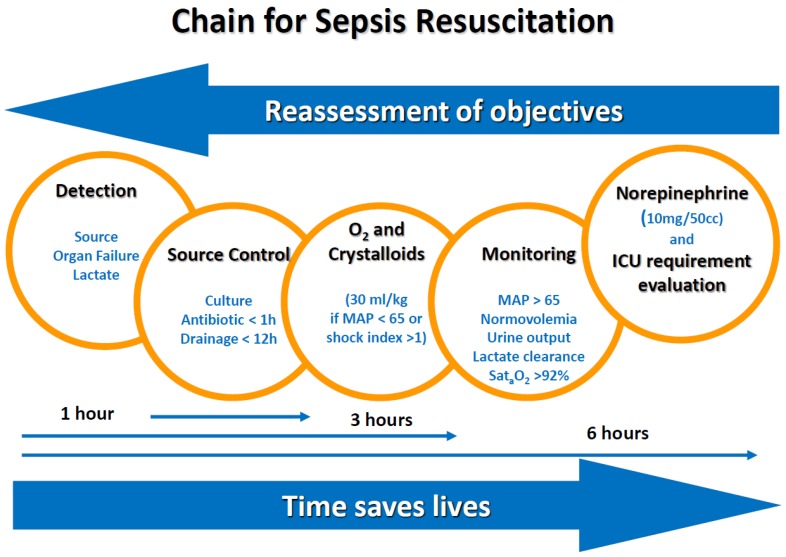
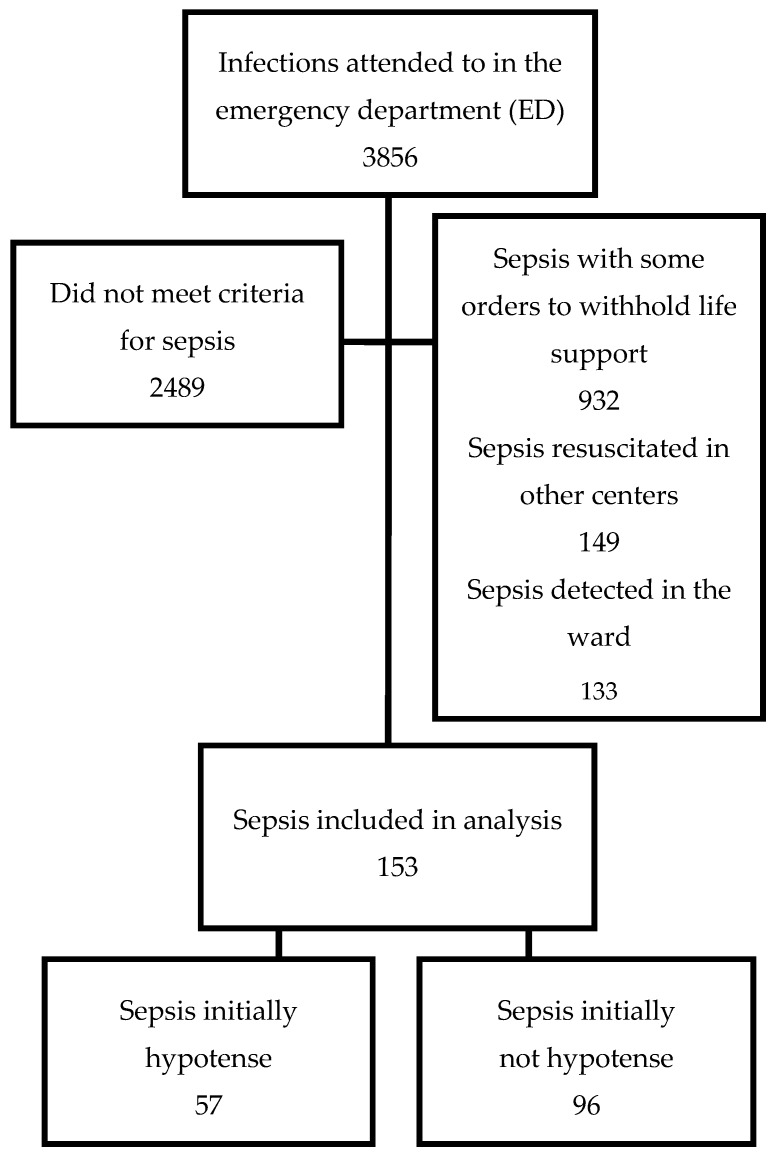
Demographic, clinical, laboratory, process of care, and outcome variables were recorded for all patients, at the emergency department of our university hospital, who presented with community-onset severe sepsis, between 1 March and 31 August in three consecutive years. Patient management consisted of standardized bundled care with five measures: Detection, blood cultures and empirical antibiotics, oxygen supplementation and fluid resuscitation (if needed), clinical monitoring, and noradrenalin administration (if needed). We compared all variables between patients who had hypotension (mean arterial pressure <65 mmHg), on admission to the emergency department, and those who did not.
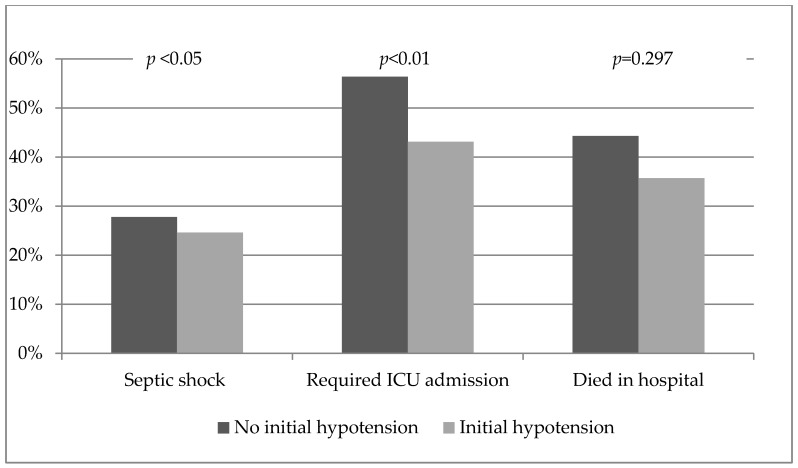
We identified 153 episodes (84 (54.5%) men; mean age 73.6 ± 1.2; mean Sequential Organ Failure Assessment (SOFA) score 4.9 ± 2.7, and 41.2% hospital mortality). Hypotension was present on admission to the emergency department in 57 patients (37.2%). Hemodynamic treatment was applied earlier in patients who presented hypotension initially. Antibiotics were administered 48 min later in non-hypotensive sepsis ( = 0.08). A higher proportion of patients without initial hypotension required admission to the intensive care unit (ICU) (43.1% for patients initially hypotensive vs. 56.9% in those initially non-hypotensive, < 0.05). Initial hypotension was not associated with mortality. A delay in door-to-antibiotic administration time was associated with mortality [OR 1.150, 95%CI: 1.043⁻1.268).
Initial management of patients with community-onset severe sepsis differed according to their clinical presentation. Initial hypotension was associated with early hemodynamic management and less ICU requirement. A non-significant delay was observed in the administration of antibiotics to initially non-hypotensive patients. The time of door-to-antibiotic administration was related to mortality.
脓毒症的诊断可能会与感染期间低血压的存在错误关联,因此非低血压性脓毒症的检测和管理可能会延迟。我们旨在评估急诊科入院时是否存在低血压如何影响社区获得性严重脓毒症患者的初始管理和预后。
连续三年的3月1日至8月31日期间,在我们大学医院急诊科对所有出现社区获得性严重脓毒症的患者记录人口统计学、临床、实验室、护理过程和预后变量。患者管理包括五项标准化综合护理措施:检测、血培养和经验性抗生素治疗、补充氧气和液体复苏(如有需要)、临床监测以及去甲肾上腺素给药(如有需要)。我们比较了急诊科入院时出现低血压(平均动脉压<65 mmHg)的患者与未出现低血压的患者之间的所有变量。
我们确定了153例病例(84例(54.5%)为男性;平均年龄73.6±1.2岁;平均序贯器官衰竭评估(SOFA)评分4.9±2.7,医院死亡率为41.2%)。急诊科入院时57例患者(37.2%)存在低血压。最初出现低血压的患者更早接受血流动力学治疗。非低血压性脓毒症患者抗生素给药时间延迟48分钟(P = 0.08)。初始无低血压的患者入住重症监护病房(ICU)的比例更高(初始低血压患者为43.1%,初始无低血压患者为56.9%,P<0.05)。初始低血压与死亡率无关。抗生素给药时间延迟与死亡率相关[比值比1.150,95%置信区间:1.043⁻1.268]。
社区获得性严重脓毒症患者的初始管理因其临床表现而异。初始低血压与早期血流动力学管理和较少的ICU需求相关。在最初无低血压的患者中,抗生素给药存在不显著的延迟。抗生素给药时间与死亡率相关。