Division of Gastroenterology, Hepatology and Nutrition, Aerodigestive Center.
Center for Airway Disorders, Department of Otolaryngology and Communication Enhancement, Boston Children's Hospital, Boston, MA.
J Pediatr Gastroenterol Nutr. 2019 Feb;68(2):218-224. doi: 10.1097/MPG.0000000000002167.
To determine if children with laryngeal penetration on videofluoroscopic swallow study (VFSS) who received feeding interventions (thickened liquids, change in liquid flow rate, and/or method of liquid delivery) had improved symptoms and decreased hospitalizations compared with those without intervention.
We performed a retrospective cohort study of children under 2 years with laryngeal penetration on VFSS at our institution in 2015 to determine initial and follow-up VFSS findings, symptom improvement at follow-up, and hospitalization risk before and after VFSS. Proportions were compared with Fisher exact test and hospitalizations with paired t tests.
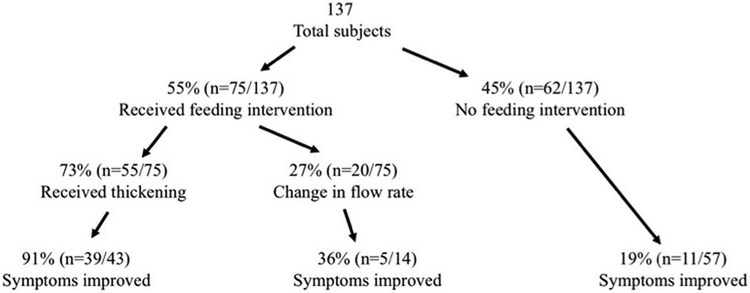
We evaluated 137 subjects with age 8.93 ± 0.59 months who had laryngeal penetration without aspiration on VFSS. Fifty-five percent had change in management, with 40% receiving thickening and 15% a change in flow rate. There was significant improvement in symptoms for children that had feeding intervention and this improvement was the greatest with thickening (OR 41.8, 95% CI 12.34-141.69, P < 0.001). On repeat VFSS, 26% had evidence of aspiration that was not captured on initial VFSS. Subjects had decreased total and pulmonary hospitalizations with feeding intervention and decreased pulmonary nights with thickening (P < 0.05).
Laryngeal penetration appears to be clinically significant in children with oropharyngeal dysphagia and interventions to decrease its occurrence are associated with improved outcomes including decreased symptoms of concern and hospitalization nights. Thickening or other feeding intervention should be considered for all symptomatic children with laryngeal penetration on swallow study.
确定在行吞咽造影检查(VFSS)时发现有喉渗透的儿童,如果接受喂养干预(增稠液体、改变液体流速和/或液体输送方式),与未接受干预的儿童相比,症状是否有所改善,住院次数是否减少。
我们对 2015 年在我院行 VFSS 检查时发现有喉渗透且年龄小于 2 岁的儿童进行了回顾性队列研究,以确定初始和随访 VFSS 结果、随访时症状改善情况以及 VFSS 前后的住院风险。使用 Fisher 精确检验比较比例,使用配对 t 检验比较住院次数。
我们评估了 137 名年龄为 8.93±0.59 个月的有喉渗透但无吸入的儿童。55%的患儿改变了治疗方案,40%接受了增稠治疗,15%改变了流速。接受喂养干预的儿童症状明显改善,增稠治疗的改善效果最大(OR 41.8,95%CI 12.34-141.69,P<0.001)。在重复 VFSS 检查中,26%的患儿有初始 VFSS 未捕捉到的吸入证据。接受喂养干预的患儿总住院次数和肺部住院次数减少,增稠治疗的肺部住院夜数减少(P<0.05)。
喉渗透在有口咽性吞咽困难的儿童中似乎具有临床意义,减少其发生的干预措施与改善结局相关,包括减轻症状和减少住院夜数。所有在吞咽研究中有喉渗透且有症状的儿童都应考虑进行增稠或其他喂养干预。