Nagahara Daigo, Fujito Takefumi, Mochizuki Atsushi, Shimoshige Shinya, Hashimoto Akiyoshi, Miura Tetsuji
Department of Cardiovascular, Renal and Metabolic Medicine Sapporo Medical University School of Medicine Sapporo Japan.
J Arrhythm. 2018 Jun 26;34(5):527-535. doi: 10.1002/joa3.12086. eCollection 2018 Oct.
Implantable cardioverter defibrillator (ICD) and cardiac resynchronization with a defibrillator (CRT-D) are established therapies for secondary prevention of sudden cardiac death (SCD) in patients with structural heart disease (SHD), but the rates of subsequent ICD/CRT-D therapy widely differ among patients with SHD. The aim of this study was to determine clinical factors associated with appropriate therapy for preventing SCD in patients with SHD.
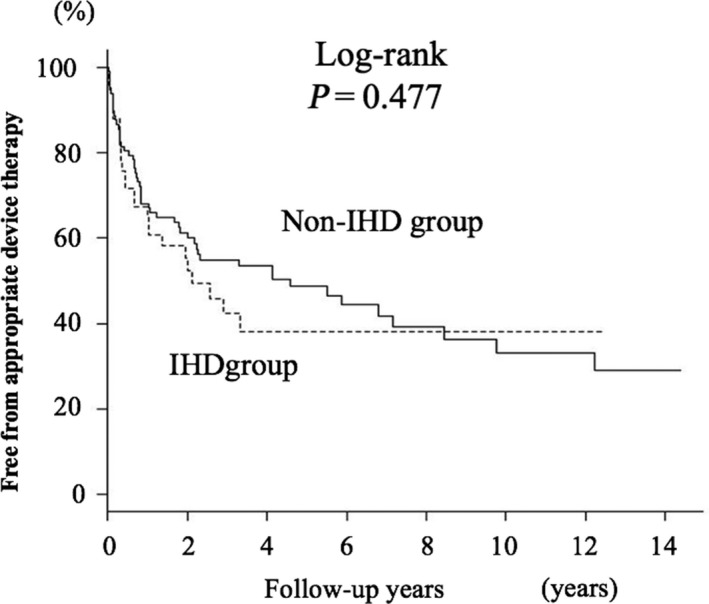
We enrolled 147 patients with SHD (mean age, 59 ± 15 years; mean ejection fraction [EF], 45 ± 15%) who underwent ICD/CRT-D implantation for secondary prevention of SCD (ischemic heart disease, n = 50; nonischemic heart disease, n = 97). ICD/CRT-D was implanted for aborted cardiopulmonary arrest (CPA, n = 65) or sustained ventricular tachycardia (VT, n = 82).
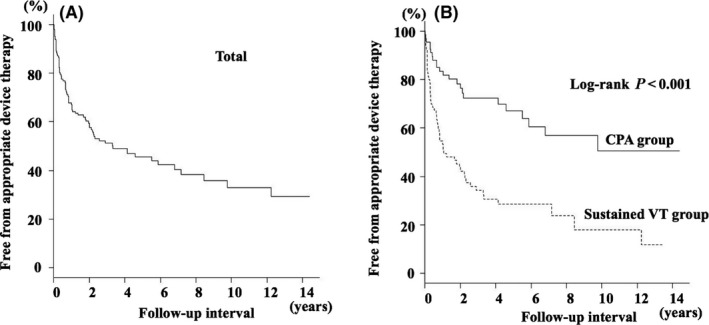
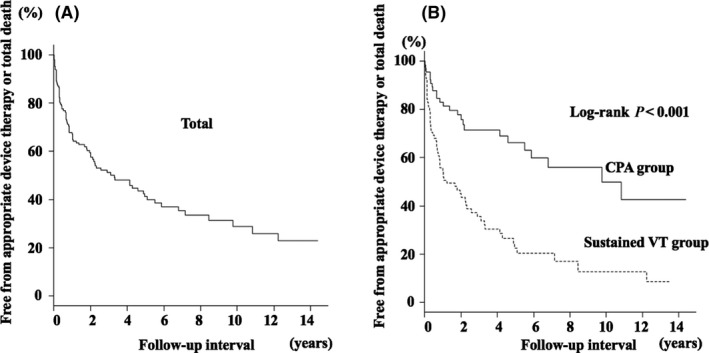
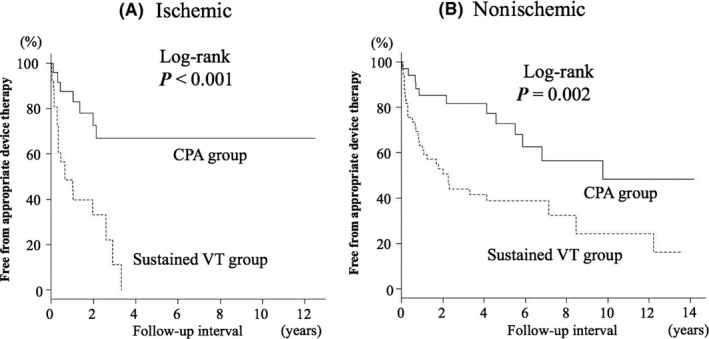
During a follow-up period of 3.2 ± 3.6 years, 79 of the 147 patients had appropriate ICD/CRT-D therapies. A Kaplan-Meier survival curve showed that the rate of appropriate therapy was 54% at 5-year follow-up. Prior sustained VT, lower EF, and use of a class I antiarrhythmic drug were significantly more frequent in patients with appropriate therapy. In multivariate analysis, prior sustained VT (hazard ratio, 2.8; 95% CI, 1.60-4.46; = .001) was the only independent predictor for appropriate ICD/CRT-D therapy. Kaplan-Meier survival curves showed that rates of appropriate therapy during a 5-year follow-up period were 70% and 34% in patients with sustained VT and those with CPA, respectively ( = .001).
In SHD patients implanted with an ICD/CRT-D, prior sustained VT as an indication of ICD/CRT-D implantation, but not EF or an antiarrhythmic drug, predicts a high rate of appropriate therapy.
植入式心脏复律除颤器(ICD)和心脏再同步化除颤器(CRT-D)是用于结构性心脏病(SHD)患者心脏性猝死(SCD)二级预防的既定疗法,但在SHD患者中,后续ICD/CRT-D治疗的发生率差异很大。本研究的目的是确定与SHD患者预防SCD的适当治疗相关的临床因素。
我们纳入了147例接受ICD/CRT-D植入以进行SCD二级预防的SHD患者(平均年龄59±15岁;平均射血分数[EF]45±15%)(缺血性心脏病,n = 50;非缺血性心脏病,n = 97)。ICD/CRT-D植入用于心脏骤停(CPA,n = 65)或持续性室性心动过速(VT,n = 82)。
在3.2±3.6年的随访期内,147例患者中有79例接受了适当的ICD/CRT-D治疗。Kaplan-Meier生存曲线显示,5年随访时适当治疗的发生率为54%。在接受适当治疗的患者中,既往持续性VT、较低的EF以及使用I类抗心律失常药物的情况明显更为常见。在多变量分析中,既往持续性VT(风险比,2.8;95%CI,1.60-4.46;P = 0.001)是适当ICD/CRT-D治疗的唯一独立预测因素。Kaplan-Meier生存曲线显示,在5年随访期内,持续性VT患者和CPA患者的适当治疗发生率分别为70%和34%(P = 0.001)。
在植入ICD/CRT-D的SHD患者中,既往持续性VT作为ICD/CRT-D植入的指征,而非EF或抗心律失常药物,可预测较高的适当治疗率。