Academic Neurosurgery Unit, Molecular and Clinical Sciences Institute, St. George's, University of London, London, SW17 0RE, UK.
Neuro-intensive Care Units, St. George's Hospital, London, UK.
Neurocrit Care. 2019 Apr;30(2):421-428. doi: 10.1007/s12028-018-0616-7.
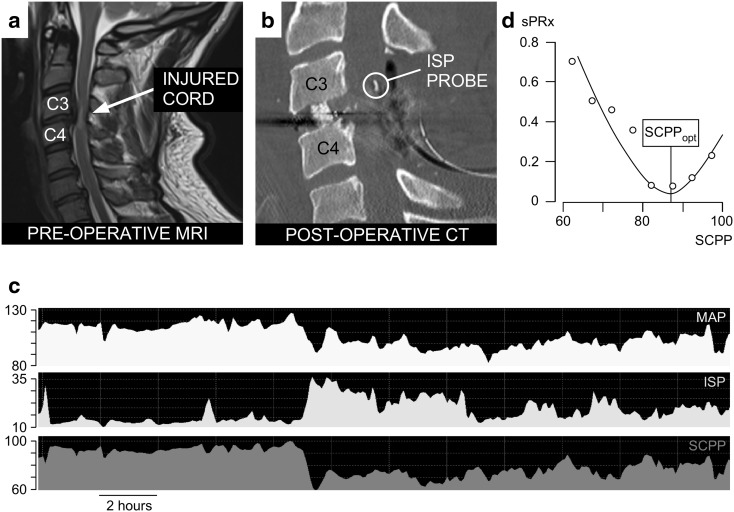
BACKGROUND/OBJECTIVES: We recently developed techniques to monitor intraspinal pressure (ISP) and spinal cord perfusion pressure (SCPP) from the injury site to compute the optimum SCPP (SCPP) in patients with acute traumatic spinal cord injury (TSCI). We hypothesized that ISP and SCPP can be predicted using clinical factors instead of ISP monitoring.
Sixty-four TSCI patients, grades A-C (American spinal injuries association Impairment Scale, AIS), were analyzed. For 24 h after surgery, we monitored ISP and SCPP and computed SCPP (SCPP that optimizes pressure reactivity). We studied how well 28 factors correlate with mean ISP or SCPP including 7 patient-related, 3 injury-related, 6 management-related, and 12 preoperative MRI-related factors.
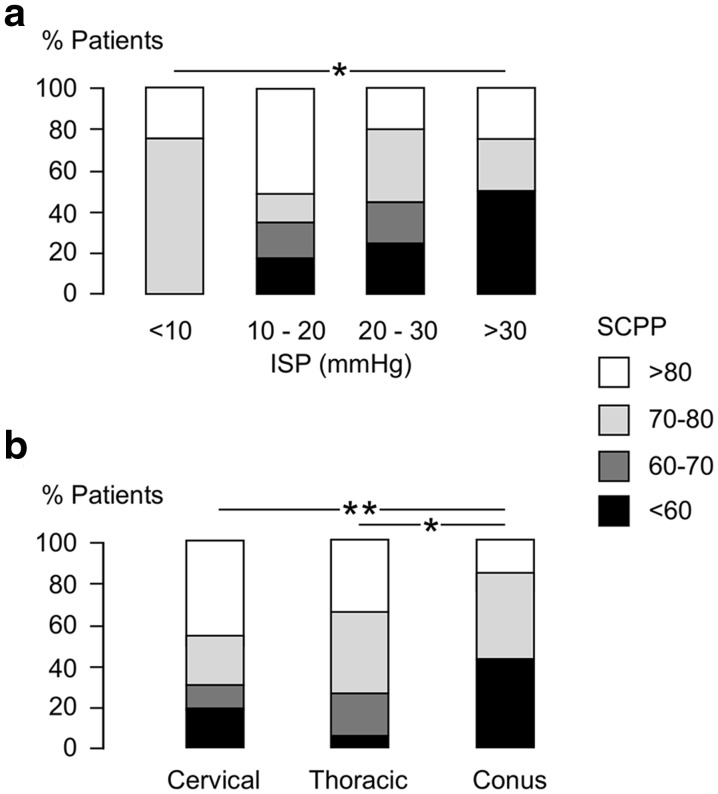
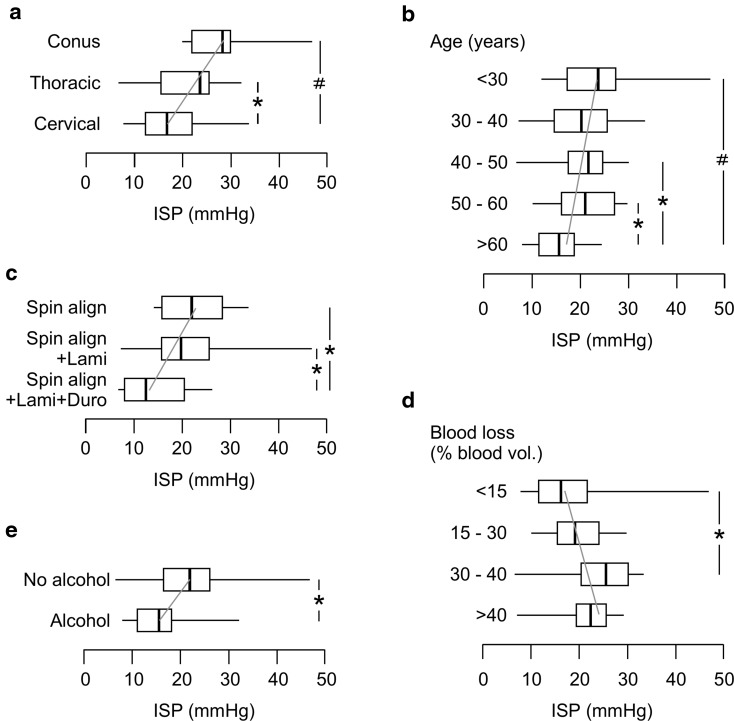
All patients underwent surgery to restore normal spinal alignment within 72 h of injury. Fifty-one percentage had U-shaped sPRx versus SCPP curves, thus allowing SCPP to be computed. Thirteen percentage, all AIS grade A or B, had no U-shaped sPRx versus SCPP curves. Thirty-six percentage (22/64) had U-shaped sPRx versus SCPP curves, but the SCPP did not reach the minimum of the curve, and thus, an exact SCPP could not be calculated. In total 5/28 factors were associated with lower ISP: older age, excess alcohol consumption, nonconus medullaris injury, expansion duroplasty, and less intraoperative bleeding. In a multivariate logistic regression model, these 5 factors predicted ISP as normal or high with 73% accuracy. Only 2/28 factors correlated with lower SCPP: higher mean ISP and conus medullaris injury. In an ordinal multivariate logistic regression model, these 2 factors predicted SCPP as low, medium-low, medium-high, or high with only 42% accuracy. No MRI factors correlated with ISP or SCPP.
Elevated ISP can be predicted by clinical factors. Modifiable factors that may lower ISP are: reducing surgical bleeding and performing expansion duroplasty. No factors accurately predict SCPP; thus, invasive monitoring remains the only way to estimate SCPP.
背景/目的:我们最近开发了从损伤部位监测椎管内压(ISP)和脊髓灌注压(SCPP)的技术,以计算急性创伤性脊髓损伤(TSCI)患者的最佳 SCPP(SCPP)。我们假设可以使用临床因素预测 ISP 和 SCPP,而无需进行 ISP 监测。
分析了 64 名 TSCI 患者(美国脊髓损伤协会损伤分级 A-C,AIS)。在手术后 24 小时内,我们监测了 ISP 和 SCPP,并计算了 SCPP(优化压力反应性的 SCPP)。我们研究了 28 个因素与平均 ISP 或 SCPP 的相关性,包括 7 个患者相关因素、3 个损伤相关因素、6 个管理相关因素和 12 个术前 MRI 相关因素。
所有患者均在损伤后 72 小时内接受手术以恢复正常脊柱排列。51%的患者具有 U 形 sPRx 与 SCPP 曲线,因此可以计算 SCPP。13%的患者,全部为 AIS 分级 A 或 B,没有 U 形 sPRx 与 SCPP 曲线。36%(22/64)具有 U 形 sPRx 与 SCPP 曲线,但 SCPP 未达到曲线的最低点,因此无法精确计算 SCPP。共有 5/28 个因素与较低的 ISP 相关:年龄较大、过量饮酒、非圆锥马尾损伤、膨胀性硬脑膜成形术和术中出血量较少。在多变量逻辑回归模型中,这 5 个因素以 73%的准确率预测 ISP 正常或较高。只有 2/28 个因素与较低的 SCPP 相关:较高的平均 ISP 和圆锥马尾损伤。在多变量有序逻辑回归模型中,这 2 个因素以 42%的准确率预测 SCPP 为低、中低、中高或高。没有 MRI 因素与 ISP 或 SCPP 相关。
较高的 ISP 可以通过临床因素预测。可能降低 ISP 的可调节因素包括减少手术出血和进行膨胀性硬脑膜成形术。没有因素能准确预测 SCPP;因此,侵入性监测仍然是估计 SCPP 的唯一方法。