Academic Neurosurgery Unit, St. George's, University of London, Cranmer Terrace, London, SW17 0RE, UK.
Neuro-anaesthesia and Neuro-intensive Care Unit, St. George's Hospital, London, SW17 0QT, UK.
Crit Care. 2023 Sep 20;27(1):362. doi: 10.1186/s13054-023-04643-y.
This study aims to determine the relationship between spinal cord perfusion pressure (SCPP) and breathing function in patients with acute cervical traumatic spinal cord injuries.
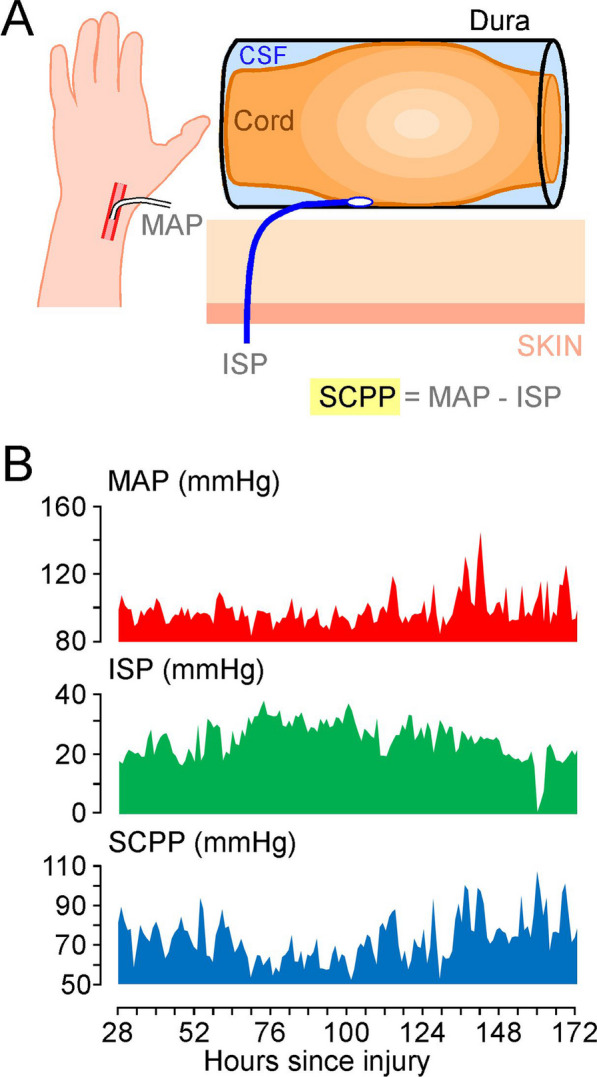
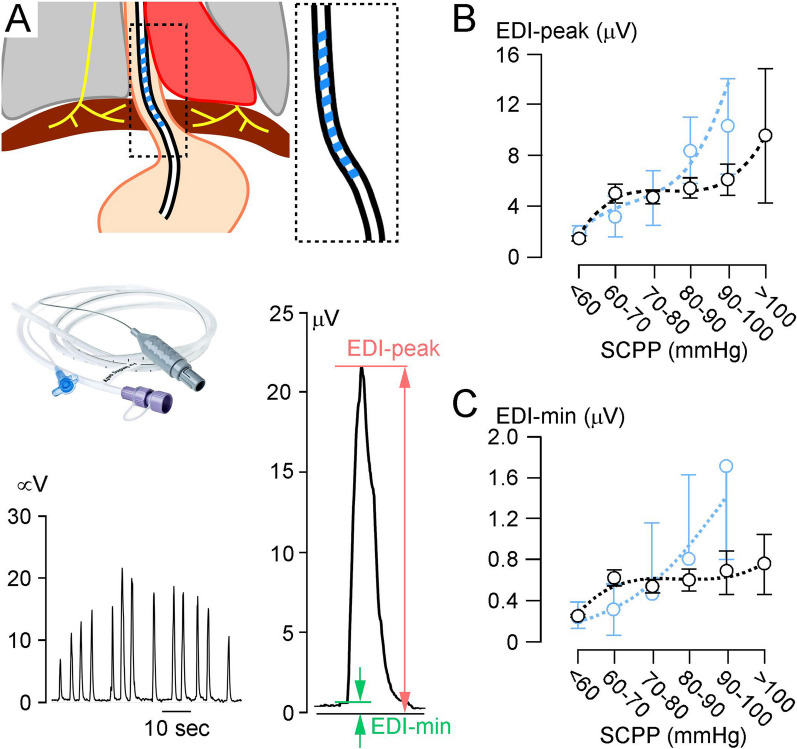
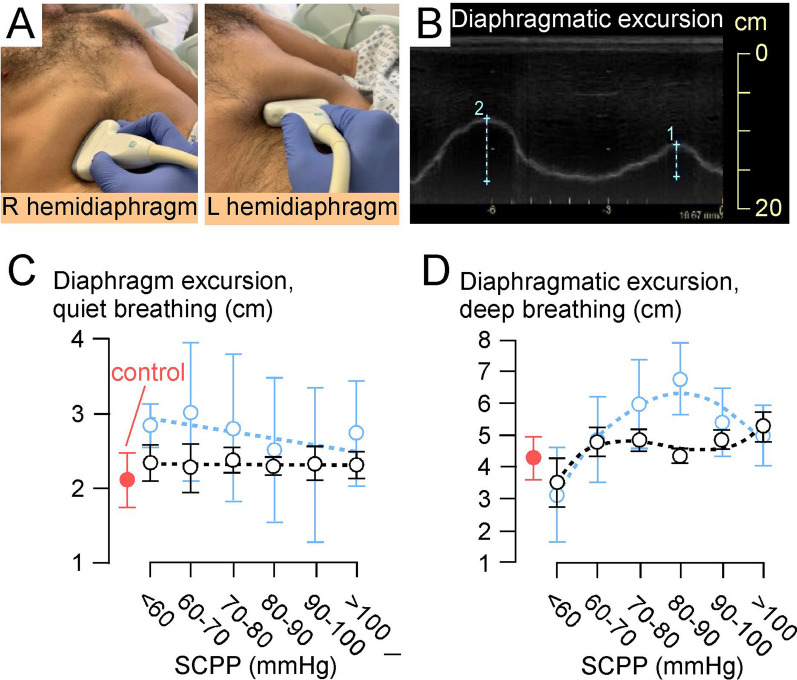
We included 8 participants without cervical TSCI plus 13 patients with cervical traumatic spinal cord injuries, American Spinal Injury Association Impairment Scale grades A-C. In the TSCI patients, we monitored intraspinal pressure from the injury site for up to a week and computed the SCPP as mean arterial pressure minus intraspinal pressure. Breathing function was quantified by diaphragmatic electromyography using an EDI (electrical activity of the diaphragm) nasogastric tube as well as by ultrasound of the diaphragm and the intercostal muscles performed when sitting at 20°-30°.
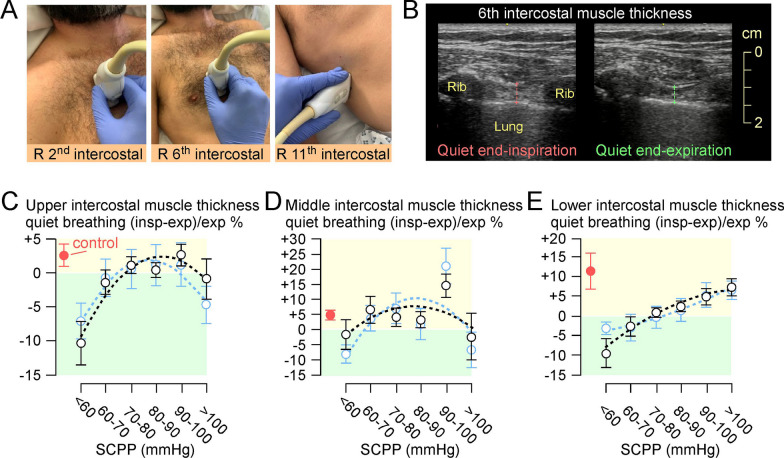
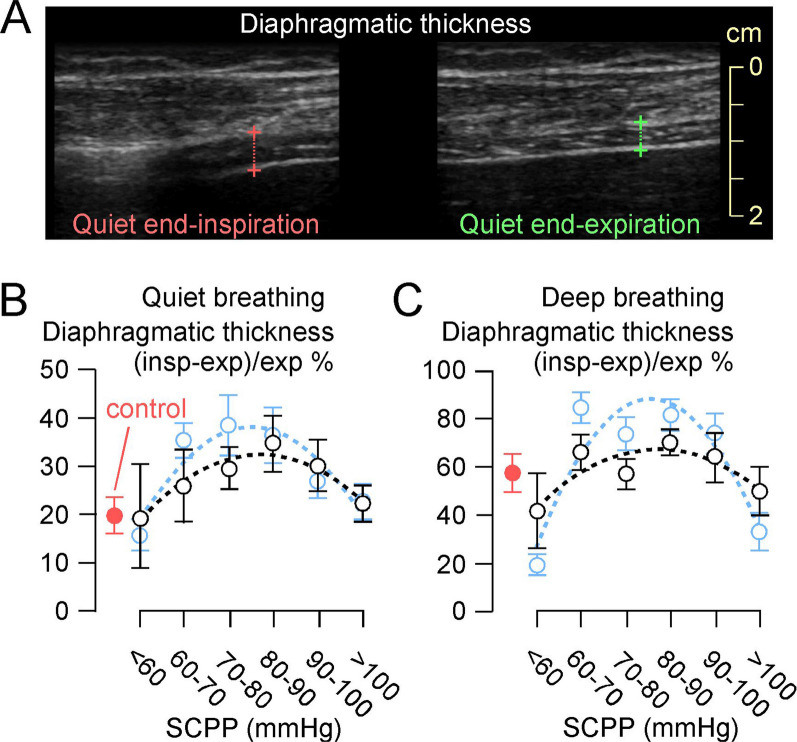
We analysed 106 ultrasound examinations (total 1370 images/videos) and 198 EDI recordings in the patients with cervical traumatic spinal cord injuries. During quiet breathing, low SCPP (< 60 mmHg) was associated with reduced EDI-peak (measure of inspiratory effort) and EDI-min (measure of the tonic activity of the diaphragm), which increased and then plateaued at SCPP 60-100 mmHg. During quiet and deep breathing, the diaphragmatic thickening fraction (force of diaphragmatic contraction) plotted versus SCPP had an inverted-U relationship, with a peak at SCPP 80-90 mmHg. Diaphragmatic excursion (up and down movement of the diaphragm) during quiet breathing did not correlate with SCPP, but diaphragmatic excursion during deep breathing plotted versus SCPP had an inverse-U relationship with a peak at SCPP 80-90 mmHg. The thickening fraction of the intercostal muscles plotted versus SCPP also had inverted-U relationship, with normal intercostal function at SCPP 80-100 mmHg, but failure of the upper and middle intercostals to contract during inspiration (i.e. abdominal breathing) at SCPP < 80 or > 100 mmHg.
After acute, cervical traumatic spinal cord injuries, breathing function depends on the SCPP. SCPP 80-90 mmHg correlates with optimum diaphragmatic and intercostal muscle function. Our findings raise the possibility that intervention to maintain SCPP in this range may accelerate ventilator liberation which may reduce stay in the neuro-intensive care unit.
本研究旨在确定急性颈外伤性脊髓损伤患者脊髓灌注压(SCPP)与呼吸功能之间的关系。
我们纳入了 8 名无颈外伤性脊髓损伤的参与者和 13 名颈外伤性脊髓损伤患者,美国脊髓损伤协会损伤分级 A-C 级。在颈外伤性脊髓损伤患者中,我们从损伤部位监测了长达一周的脊髓内压,并计算了平均动脉压减去脊髓内压的 SCPP。呼吸功能通过 EDI(膈肌电活动)鼻胃管以膈肌肌电图和 20°-30°坐位时的膈肌和肋间肌超声进行量化。
我们分析了 106 例颈外伤性脊髓损伤患者的 198 次 EDI 记录和 1370 张超声图像/视频。在安静呼吸时,低 SCPP(<60mmHg)与 EDI-峰值(吸气努力的测量)和 EDI-最小(膈肌紧张活动的测量)降低相关,随后在 SCPP 60-100mmHg 时增加并达到平台。在安静和深呼吸时,膈肌增厚分数(膈肌收缩力)与 SCPP 的关系呈倒 U 型,在 SCPP 80-90mmHg 时达到峰值。安静呼吸时的膈肌运动(膈肌上下运动)与 SCPP 无相关性,但深呼吸时的膈肌运动与 SCPP 的关系呈倒 U 型,在 SCPP 80-90mmHg 时达到峰值。肋间肌增厚分数与 SCPP 的关系也呈倒 U 型,SCPP 80-100mmHg 时肋间肌功能正常,但 SCPP<80mmHg 或>100mmHg 时,上中肋间肌不能收缩(即腹式呼吸)。
颈外伤性脊髓损伤后,呼吸功能取决于 SCPP。SCPP 80-90mmHg 与最佳膈肌和肋间肌功能相关。我们的发现提示,维持 SCPP 在该范围内可能会加速呼吸机撤离,从而减少神经重症监护病房的停留时间。