Ballester-Clau Raquel, Torres Vicente Gisela, Voltà-Pardo Tania, López-Barroso Laura, Cucala-Ramos Mercedes, Reñé-Espinet Josep M, Planella de Rubinat Montse
Department of Gastroenterology, Arnau de Vilanova University Hospital.
Institute for Biomedical Research in Lleida Dr. Pifarré Foundation, IRB Lleida, Lleida.
Eur J Gastroenterol Hepatol. 2019 Jan;31(1):116-122. doi: 10.1097/MEG.0000000000001282.
The aim of this study was to assess the efficacy and safety of intravenous ferric carboxymaltose (FCM) following hospitalization for acute gastrointestinal bleeding (AGIB) in the context of a restrictive transfusion strategy.
A retrospective single-center study analyzed patients with AGIB (excluding AGIB secondary to portal hypertension) administered a single FCM dose with or without blood transfusion.
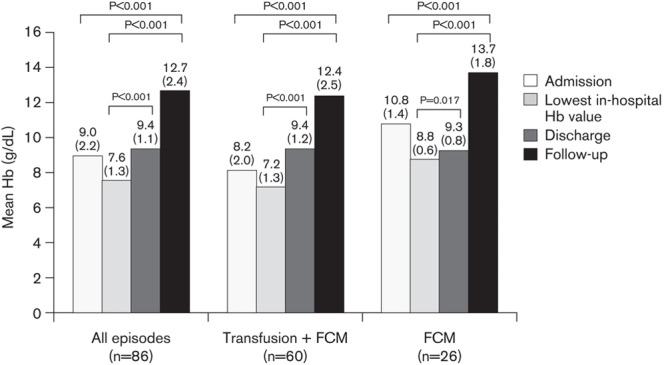
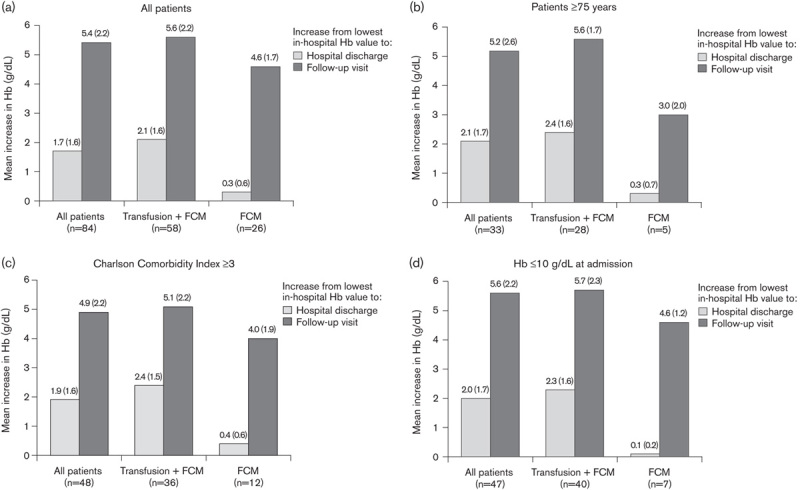
Eighty-six episodes in 84 patients were analyzed. Seventy-nine patients had upper AGIB. Nineteen episodes were associated with hemodynamic instability. FCM was administered during hospitalization as a single dose of 1000 mg iron in 84/86 episodes and as a single dose of 500 mg iron in two episodes, with blood transfusion in 60/86 (69.8%) episodes. The mean hemoglobin (Hb) was 9.0 g/dl at admission, 7.6 g/dl at the lowest in-hospital value, 9.4 g/dl at discharge, and 12.7 g/dl at follow-up (mean: 55 days postdischarge) (P<0.001 for follow-up vs. all other timepoints). The lowest mean in-hospital Hb value was 7.2 and 8.8 g/dl, respectively, in patients with transfusion+FCM versus FCM alone; the mean Hb was 12.4 versus 13.7 g/dl at follow-up. In patients administered FCM alone, the mean Hb at follow-up in the subpopulations aged older than or equal to 75 years (n=33), Charlson comorbidity index of at least 3 (n=48), and Hb of up to 10 g/dl at admission (n=47) were 12.6, 13.1, and 13.3 g/dl, respectively. No adverse effects were detected.
Treatment with FCM for AGIB is associated with a good erythropoietic response and anemia correction after hospitalization, even in severe episodes or when transfusion is needed. FCM is safe and well tolerated, and may support a restrictive transfusion policy.
本研究旨在评估在限制性输血策略背景下,急性胃肠道出血(AGIB)住院后静脉注射羧基麦芽糖铁(FCM)的疗效和安全性。
一项回顾性单中心研究分析了接受单次FCM剂量治疗且有或无输血的AGIB患者(不包括门静脉高压继发的AGIB)。
分析了84例患者的86次发作情况。79例患者为上消化道AGIB。19次发作与血流动力学不稳定有关。在86次发作中的84次,住院期间给予FCM单次剂量为1000mg铁,2次发作给予单次剂量500mg铁,60/86(69.8%)次发作进行了输血。入院时平均血红蛋白(Hb)为9.0g/dl,住院期间最低值为7.6g/dl,出院时为9.4g/dl,随访时(出院后平均55天)为12.7g/dl(随访与所有其他时间点相比,P<0.001)。输血联合FCM组与单纯FCM组患者住院期间最低平均Hb值分别为7.2和8.8g/dl;随访时平均Hb分别为12.4和13.7g/dl。在单纯接受FCM治疗的患者中,年龄大于或等于75岁亚组(n = 33)、Charlson合并症指数至少为3亚组(n = 48)以及入院时Hb最高达10g/dl亚组(n = 47)随访时的平均Hb分别为12.6、13.1和13.3g/dl。未检测到不良反应。
即使在严重发作或需要输血的情况下,AGIB患者接受FCM治疗后住院期间红细胞生成反应良好且贫血得到纠正。FCM安全且耐受性良好,可能支持限制性输血策略。