De Mattia Elena, Dreussi Eva, Montico Marcella, Gagno Sara, Zanusso Chiara, Quartuccio Luca, De Vita Salvatore, Guardascione Michela, Buonadonna Angela, D'Andrea Mario, Pella Nicoletta, Favaretto Adolfo, Mini Enrico, Nobili Stefania, Romanato Loredana, Cecchin Erika, Toffoli Giuseppe
Experimental and Clinical Pharmacology Unit, CRO Aviano National Cancer Institute, Istituto di Ricovero e Cura a Carattere Scientifico, Aviano, Italy.
Scientific Directorate, Centro di Riferimento Oncologico di Aviano (CRO), IRCCS, Aviano, Italy.
Front Pharmacol. 2018 Oct 4;9:1101. doi: 10.3389/fphar.2018.01101. eCollection 2018.
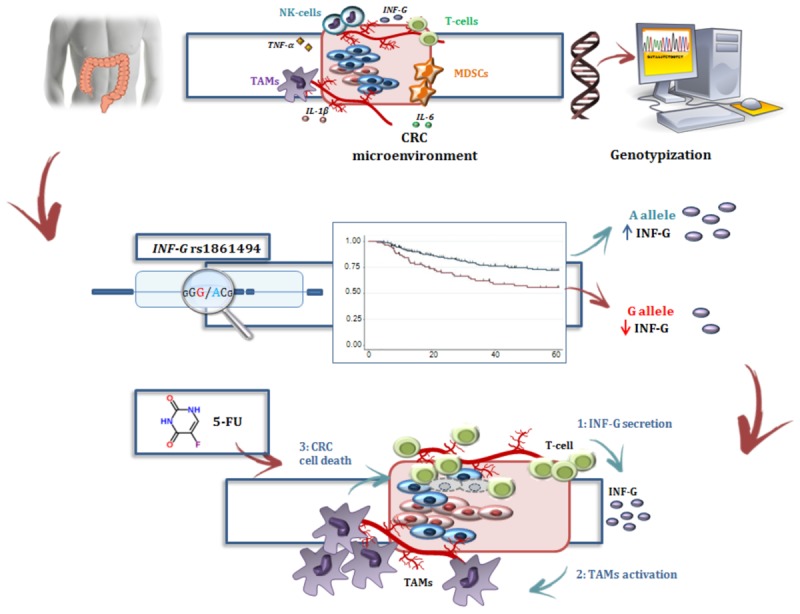
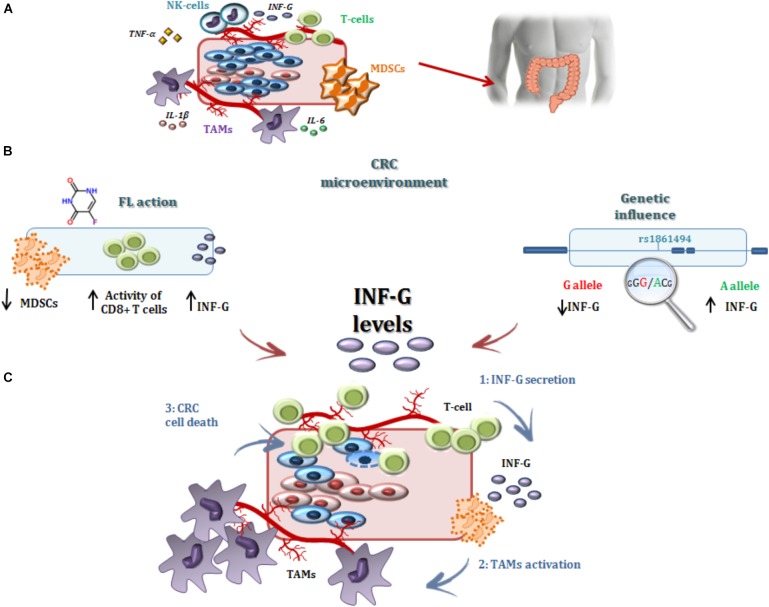
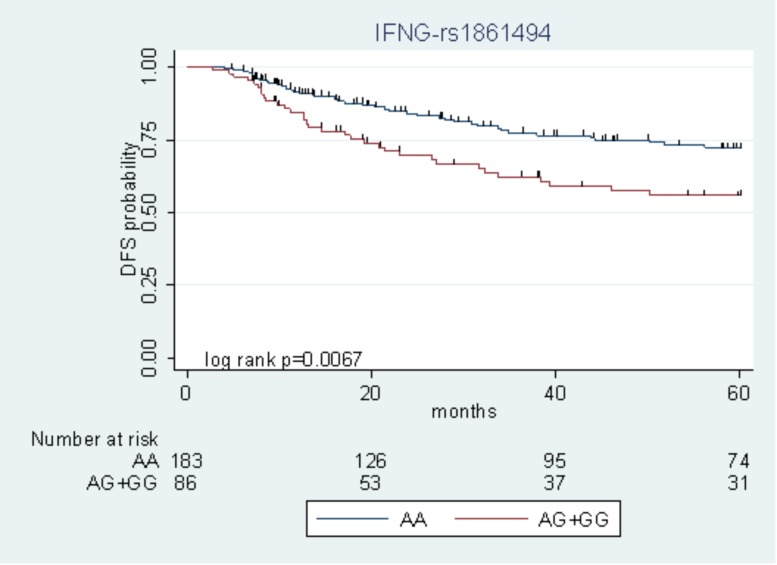
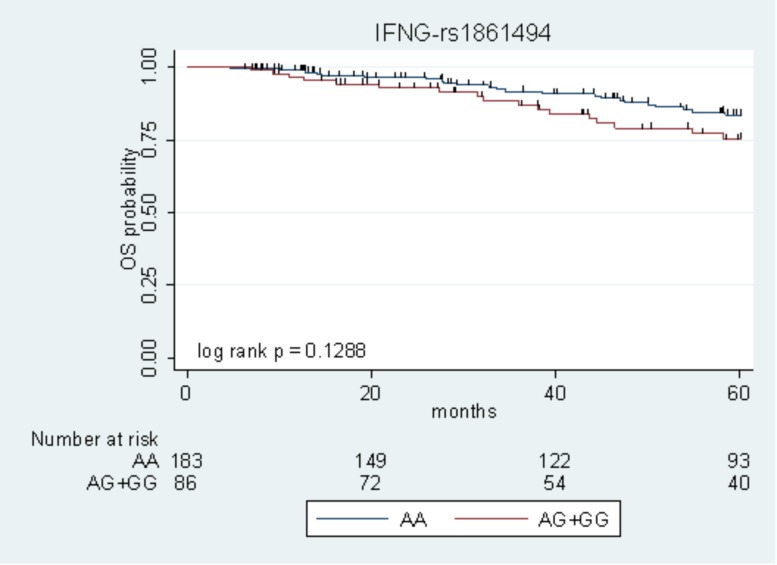
There are clinical challenges related to adjuvant treatment in colorectal cancer (CRC) and novel molecular markers are needed for better risk stratification of patients. Our aim was to integrate our previously reported clinical-genetic prognostic score with new immunogenetic markers of 5-year disease-free survival (DFS) to evaluate the recurrence risk stratification before fluoropyrimidine (FL)-based adjuvant therapy. The study population included a total of 270 stage II-III CRC patients treated with adjuvant FL with (FL + OXA, = 119) or without oxaliplatin (FL, = 151). Patients were genotyped for a panel of 192 tagging polymorphisms in 34 immune-related genes. The -rs1861494 polymorphism was associated with worse DFS in the FL + OXA (HR = 2.14, 95%CI 1.13-4.08; = 0.020, -value = 0.249) and FL (HR = 1.97, 95%CI 1.00-3.86; = 0.049) cohorts, according to a dominant model. The integration of -rs1861494 in our previous clinical genetic multiparametric score of DFS improved the patients' risk stratification (Log-rank = 0.0026 in the pooled population). These findings could improve the discrimination of patients who would benefit from adjuvant treatment. In addition, the results may help better elucidate the interplay between the immune system and chemotherapeutics and help determine the efficacy of anti-tumor strategies.
结直肠癌(CRC)辅助治疗存在临床挑战,需要新的分子标志物来更好地对患者进行风险分层。我们的目的是将我们之前报道的临床遗传预后评分与5年无病生存期(DFS)的新免疫遗传标志物相结合,以评估基于氟嘧啶(FL)的辅助治疗前的复发风险分层。研究人群包括总共270例接受辅助FL治疗的II-III期CRC患者,其中接受(FL + OXA,n = 119)或不接受奥沙利铂(FL,n = 151)治疗。对患者进行了34个免疫相关基因中192个标签多态性的基因分型。根据显性模型,-rs1861494多态性与FL + OXA(HR = 2.14,95%CI 1.13-4.08;P = 0.020,I²值 = 0.249)和FL(HR = 1.97,95%CI 1.00-3.86;P = 0.049)队列中较差的DFS相关。将-rs1861494纳入我们之前的DFS临床遗传多参数评分中可改善患者的风险分层(合并人群中Log-rank P = 0.0026)。这些发现可改善对将从辅助治疗中获益的患者的鉴别。此外,结果可能有助于更好地阐明免疫系统与化疗药物之间的相互作用,并有助于确定抗肿瘤策略的疗效。