Fitchett David H
Division of Cardiology, St Michael's Hospital, University of Toronto, Ontario, Canada.
Eur Endocrinol. 2018 Sep;14(2):40-49. doi: 10.17925/EE.2018.14.2.40. Epub 2018 Sep 10.
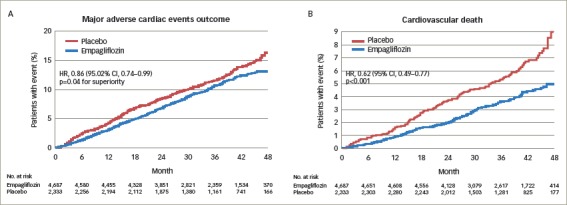
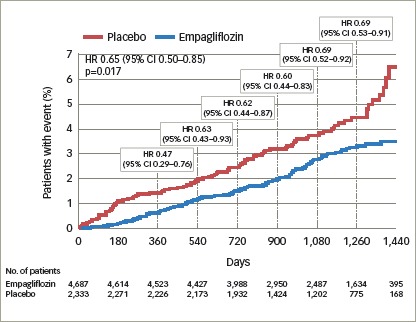
In patients with type 2 diabetes (T2D), the excretion of glucose by the kidney with sodium-glucose cotransporter 2 (SGLT2) inhibitors lowers glycosylated haemoglobin (HbA1c) levels, decreases body weight and visceral adiposity, as well as improving cardio-renal haemodynamics. Currently, four SGLT2 inhibitors are approved in the US and Europe to improve glycaemic control - empagliflozin, dapagliflozin, canagliflozin, and ertuglifozin. Recently, the SGLT2 inhibitor empagliflozin was approved by the FDA for the reduction of cardiovascular (CV) death in adults with T2D and CV disease (CVD). This approval was based on the findings of the Empagliflozin, Cardiovascular Outcomes, and Mortality in Type 2 Diabetes (EMPA-REG OUTCOME) study, which was the first study to show a significant reduction of a primary CV endpoint with a glucose-lowering agent. In this study, the primary outcome (CV mortality, non-fatal myocardial infarction [MI] and non-fatal stroke) was reduced by empagliflozin (10.5%; 490/4,687) compared with placebo (12.1%; 282/2,333); hazard ratio (HR), 0.86 (95% confidence interval [CI]: 0.74, 0.99). The primary outcome was driven by a large reduction of CV mortality (relative risk reduction [RRR], 38%). Empagliflozin also reduced all-cause mortality (RRR, 32%). Furthermore, empagliflozin reduced the adjudicated outcome of heart failure (HF) hospitalisation by 35% (HR, 0.65; 95% CI: 0.50, 0.85). Other non-adjudicated measures of HF outcomes were similarly reduced including investigator reported HF, the introduction of loop diuretics and death from HF. In the analysis of renal outcomes, incident or worsening nephropathy was reduced for empagliflozin (12.7%) compared with placebo (18.8%); HR, 0.61 (95% CI: 0.53, 0.70). Empagliflozin significantly reduced the risk of progression to macroalbuminuria (38%) and doubling of creatinine (44%), as well as the need of starting renal-replacement therapy (55%). The benefits of empagliflozin for the reduction of CV death, all-cause death and hospitalisation for HF were observed across a range of baseline subgroups such as HbA1c level and renal function (down to estimated glomerular filtration rate [eGFR] 30 ml/min/1.73 m). The rapid reduction of HF outcomes with empagliflozin is observed across the spectrum of CVD and HF risk and represents a therapeutic advance in the prevention and perhaps also in the treatment of HF, an often poorly recognised complication of T2D. This review discusses the EMPA-REG OUTCOME study and the implications for treating patients with T2D and CVD.
在2型糖尿病(T2D)患者中,使用钠-葡萄糖协同转运蛋白2(SGLT2)抑制剂促使肾脏排泄葡萄糖可降低糖化血红蛋白(HbA1c)水平,减轻体重和内脏脂肪,还能改善心肾血流动力学。目前,美国和欧洲已批准四种SGLT2抑制剂用于改善血糖控制,分别是恩格列净、达格列净、卡格列净和依鲁格列净。最近,SGLT2抑制剂恩格列净获美国食品药品监督管理局(FDA)批准,用于降低患有T2D和心血管疾病(CVD)的成人的心血管(CV)死亡风险。这一批准基于恩格列净、心血管结局和2型糖尿病死亡率(EMPA-REG OUTCOME)研究的结果,该研究是首个显示降糖药物能显著降低主要CV终点事件的研究。在这项研究中,与安慰剂组(12.1%;282/2333)相比,恩格列净使主要结局(CV死亡率、非致死性心肌梗死[MI]和非致死性卒中)降低(10.5%;490/4687);风险比(HR)为0.86(95%置信区间[CI]:0.74,0.99)。主要结局的改善主要得益于CV死亡率的大幅降低(相对风险降低率[RRR]为38%)。恩格列净还降低了全因死亡率(RRR为32%)。此外,恩格列净使判定的心力衰竭(HF)住院结局降低了35%(HR为0.65;95%CI:0.50,0.85)。其他未判定的HF结局指标也有类似程度的降低,包括研究者报告的HF、袢利尿剂的使用以及HF导致的死亡。在肾脏结局分析中,与安慰剂组(18.8%)相比,恩格列净使新发或恶化的肾病减少(12.7%);HR为0.61(95%CI:0.53,0.70)。恩格列净显著降低了进展为大量蛋白尿的风险(38%)、肌酐翻倍的风险(44%)以及开始肾脏替代治疗的需求(55%)。在一系列基线亚组中,如HbA1c水平和肾功能(低至估计肾小球滤过率[eGFR]30 ml/min/1.73 m²),均观察到恩格列净在降低CV死亡、全因死亡和HF住院方面的益处。在整个CVD和HF风险范围内,均观察到恩格列净能迅速改善HF结局,这代表在预防甚至可能在治疗HF方面取得了治疗进展,HF是T2D一种常被忽视的并发症。本综述讨论了EMPA-REG OUTCOME研究以及对治疗T2D和CVD患者的意义。