Center for Alcohol and Addictions Studies, Brown University School of Public Health, United States of America.
Center for Alcohol and Addictions Studies, Brown University School of Public Health, United States of America.
J Subst Abuse Treat. 2018 Dec;95:26-34. doi: 10.1016/j.jsat.2018.09.004. Epub 2018 Sep 11.
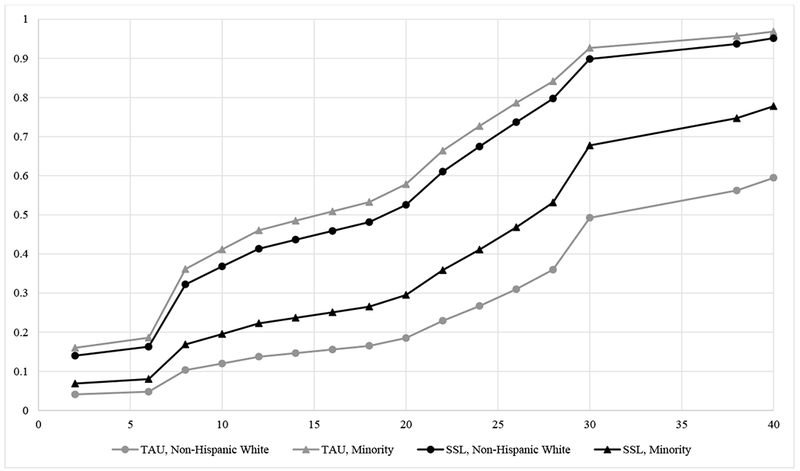
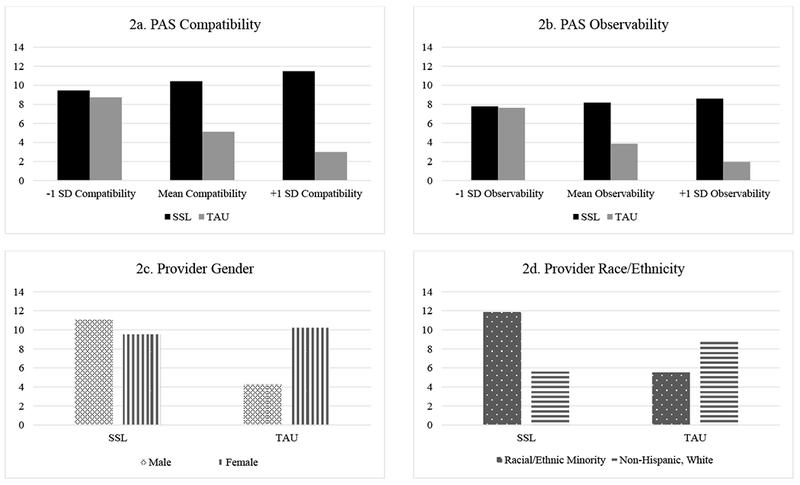
Contingency management (CM) is a well-established treatment for opioid use, yet its adoption remains low in community clinics. This manuscript presents a secondary analysis of a study comparing a comprehensive implementation strategy (Science to Service Laboratory; SSL) to didactic training-as-usual (TAU) as a means of implementing CM across a multi-site opioid use disorder program. Hypotheses predicted that providers who received the SSL implementation strategy would 1) adopt CM faster and 2) deliver CM more frequently than TAU providers. In addition, we examined whether the effect of implementation strategy varied as a function of a set of theory-driven moderators, guided by the Consolidated Framework for Implementation Research: perceived intervention characteristics, perceived organizational climate, and provider characteristics (i.e., race/ethnicity, gender). Sixty providers (39 SSL, 21 TAU) across 15 clinics (7 SSL, 8 TAU) completed a comprehensive set of measures at baseline and reported biweekly on CM use for 52 weeks. All participants received didactic CM training; SSL clinics received 9 months of enhanced training, including access to an external coach, an in-house innovation champion, and a collaborative learning community. Discrete-time survival analysis found that SSL providers more quickly adopted CM; provider characteristics (i.e., race/ethnicity) emerged as the sole moderator of time to adoption. Negative binomial regression revealed that SSL providers also delivered CM more frequently than TAU providers. Frequency of CM adoption was moderated by provider (i.e., gender and race/ethnicity) and intervention characteristics (i.e., compatibility). Implications for implementation strategies for community-based training are discussed.
contingency management (CM) 是一种经过充分验证的治疗阿片类药物使用的方法,但在社区诊所中的采用率仍然很低。本文对一项研究进行了二次分析,该研究比较了一种综合实施策略(Science to Service Laboratory;SSL)与常规教学培训(TAU),以将 CM 应用于多站点阿片类药物使用障碍项目。假设预测,接受 SSL 实施策略的提供者将 1)更快地采用 CM,2)比 TAU 提供者更频繁地提供 CM。此外,我们还检查了实施策略的效果是否因一组理论驱动的调节剂而有所不同,这些调节剂由实施研究综合框架指导:干预措施的感知特征、感知组织氛围以及提供者特征(即种族/族裔、性别)。15 个诊所中的 60 名提供者(39 名 SSL,21 名 TAU)完成了一套全面的基线措施,并在 52 周内每两周报告一次 CM 使用情况。所有参与者都接受了 CM 教学培训;SSL 诊所接受了 9 个月的强化培训,包括获得外部教练、内部创新冠军和协作学习社区。离散时间生存分析发现,SSL 提供者更快地采用了 CM;提供者特征(即种族/族裔)是采用时间的唯一调节剂。负二项回归显示,SSL 提供者提供 CM 的频率也高于 TAU 提供者。CM 采用的频率由提供者(即性别和种族/族裔)和干预特征(即兼容性)调节。讨论了基于社区的培训实施策略的含义。