Institute of Infection and Global Health, University of Liverpool, Liverpool, UK.
Karonga Prevention Study, Chilumba, Malawi.
Vaccine. 2018 Nov 19;36(48):7369-7376. doi: 10.1016/j.vaccine.2018.10.021. Epub 2018 Oct 21.
Thirteen-valent pneumococcal conjugate vaccine (PCV13) was introduced in Malawi in November 2011 and is offered to infants at 6, 10 and 14 weeks of age as part of routine immunisation. PCV13 is expected to reduce vaccine type (VT) nasopharyngeal carriage, leading to reduced transmission and herd protection.
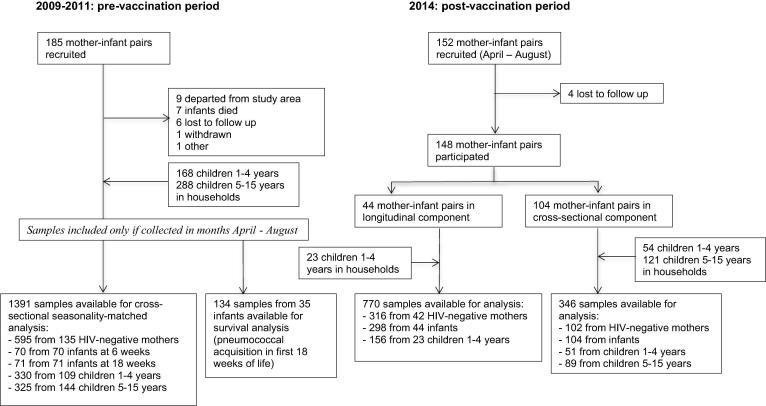
We compared pneumococcal carriage in rural Karonga District, Malawi, pre-vaccine in 2009-2011 and post-vaccine in 2014 using a combination of cross-sectional and longitudinal analyses. Nasopharyngeal swabs were collected from a cohort of mother-infant pairs and household members <16 years. Pneumococci from 2009 to 2011 were serogrouped using latex agglutination and serotyped by Quellung reaction. In 2014, latex agglutination was used for both steps. Carriage prevalence ratios using prevalence data from before and after vaccine introduction were calculated by log-binomial regression, adjusted for age, seasonality and household composition. Participating infants in 2014 received PCV13 as part of routine immunisation.
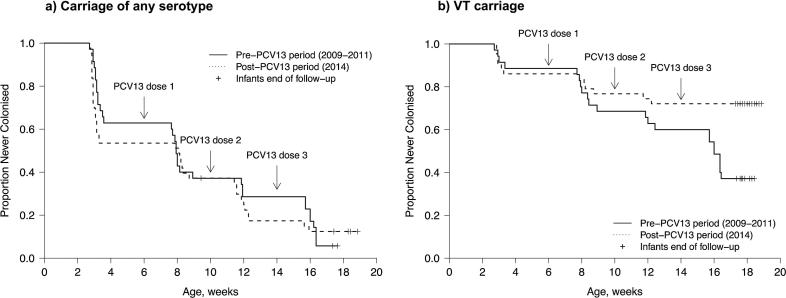
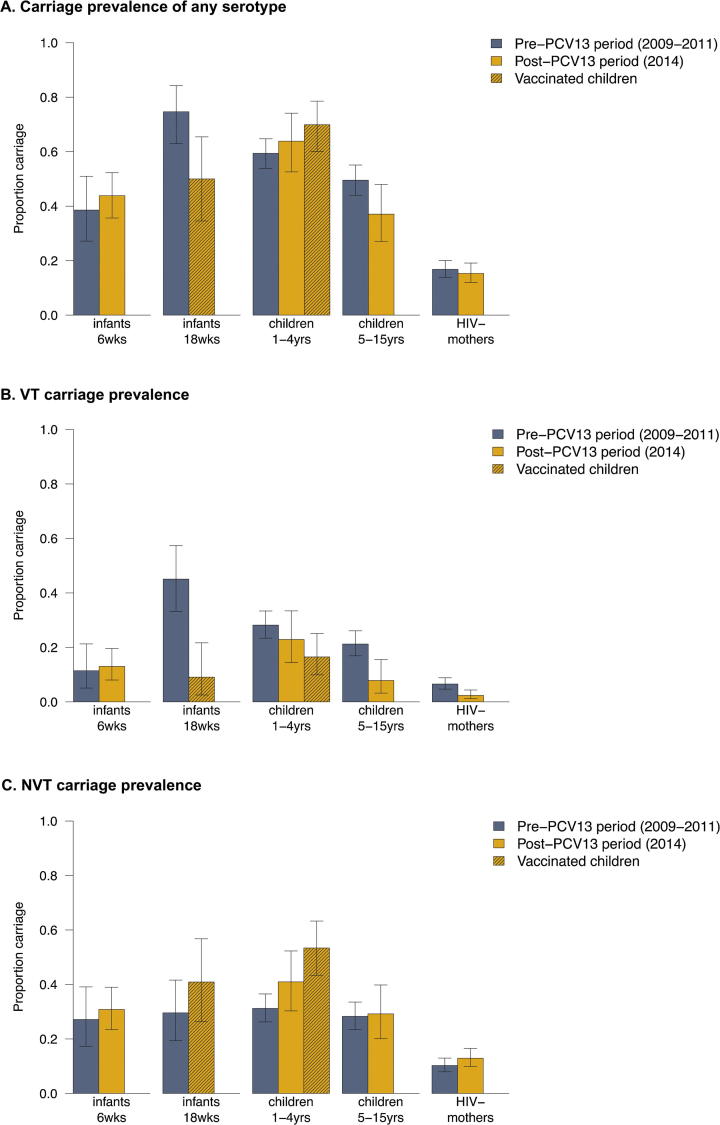
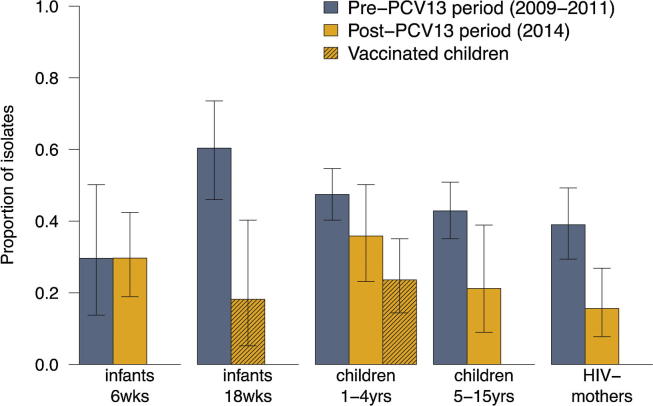
VT carriage prior to PCV-13 introduction was 11.4%, 45.1%, 28.2%, 21.2% and 6.6% for 6-week old infants, 18-week old infants, children 1-4 years, children 5-15 years and mothers, respectively. After vaccine introduction, VT carriage decreased among vaccinated 18-week old infants (adjusted prevalence ratio 0.24 (95%CI 0.08-0.75)), vaccinated children 1-4 years (0.54 (0.33-0.88)), unvaccinated children 5-15 years (0.37 (0.17-0.78)) and mothers (0.34 (0.15-0.79)). No decrease in VT carriage was observed for 6-week old infants too young to be vaccinated (1.07 (0.38-3.02)) and PCV-13 ineligible children 1-4 years (0.84 (0.53-1.33)). Non-VT carriage increased only among vaccinated children 1-4 years (1.58 (1.21-2.06)).
There is evidence of reduced VT pneumococcal carriage three years after vaccine introduction in this rural Malawian population with good vaccine coverage using a 3 + 0 schedule. However carriage was sustained among 6-week-old infants and PCV13 ineligible 1-4 year olds, and there was some indication of serotype replacement in vaccinated 1-4 year olds.
十三价肺炎球菌结合疫苗(PCV13)于 2011 年 11 月在马拉维引入,并作为常规免疫的一部分,在婴儿 6、10 和 14 周龄时提供。PCV13 有望降低疫苗型(VT)鼻咽携带率,从而降低传播和群体保护。
我们比较了 2009-2011 年疫苗前和 2014 年疫苗后的马拉维卡隆加区农村的肺炎球菌携带情况,使用了横断面和纵向分析相结合的方法。从母婴对和<16 岁的家庭成员中采集鼻咽拭子。2009 年至 2011 年的肺炎球菌通过乳胶凝集法进行血清群分类,并用 Quellung 反应进行血清分型。2014 年,乳胶凝集法用于这两个步骤。使用疫苗引入前后的患病率数据计算携带率比,采用对数二项式回归进行调整,以年龄、季节性和家庭构成作为调整因素。2014 年参与的婴儿作为常规免疫的一部分接种了 PCV13。
在 PCV-13 引入之前,6 周龄婴儿、18 周龄婴儿、1-4 岁儿童、5-15 岁儿童和母亲的 VT 携带率分别为 11.4%、45.1%、28.2%、21.2%和 6.6%。疫苗引入后,接种 18 周龄婴儿的 VT 携带率下降(调整后患病率比 0.24(95%CI 0.08-0.75))、接种 1-4 岁儿童(0.54(0.33-0.88))、未接种 5-15 岁儿童(0.37(0.17-0.78))和母亲(0.34(0.15-0.79))。未观察到接种疫苗的 6 周龄婴儿(太小不能接种疫苗)和接种疫苗的 1-4 岁儿童(PCV-13 不适用)的 VT 携带率下降(1.07(0.38-3.02)和 0.84(0.53-1.33))。非 VT 携带率仅在接种疫苗的 1-4 岁儿童中增加(1.58(1.21-2.06))。
在马拉维农村地区,使用 3+0 免疫程序,在良好的疫苗覆盖率下,疫苗引入三年后,有证据表明 VT 肺炎球菌携带率降低。然而,6 周龄婴儿和 PCV13 不适用的 1-4 岁儿童的携带率仍持续存在,接种疫苗的 1-4 岁儿童中存在一些血清型替代的迹象。