From the Department of Neurology (H.J.F., N.K.H.), University of California, San Francisco.
Department of Pediatrics (H.J.F.), University of California, San Francisco.
Stroke. 2018 Nov;49(11):2590-2596. doi: 10.1161/STROKEAHA.118.021556.
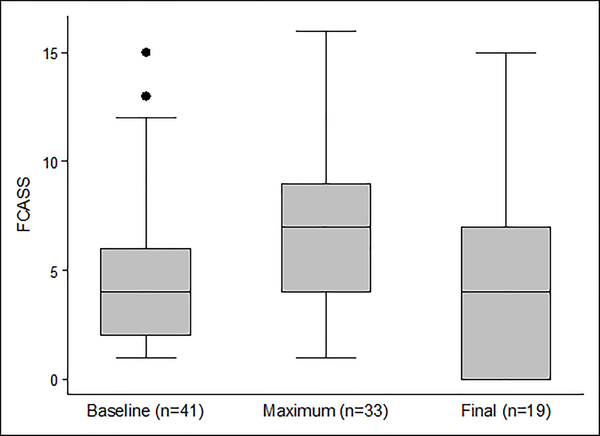
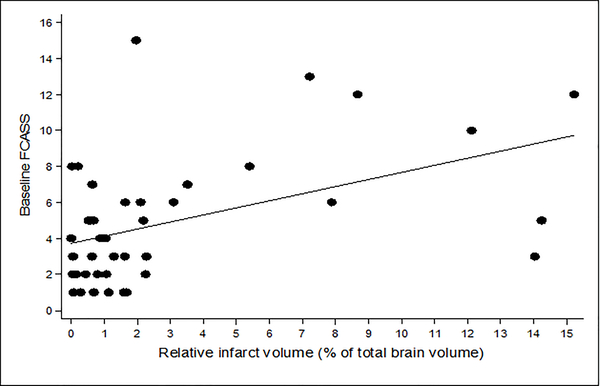
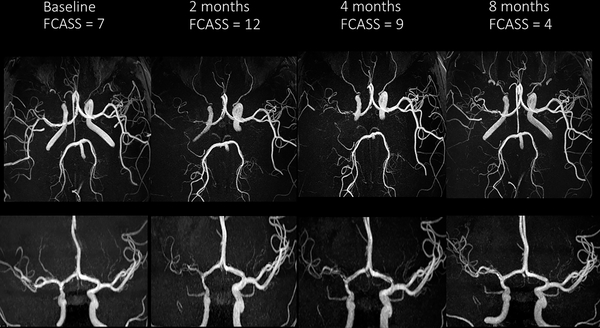
Background and Purpose- Focal cerebral arteriopathy (FCA)-a common cause of arterial ischemic stroke in previously healthy children-often progresses over days to weeks, increasing the risk of recurrent stroke. We developed a novel severity scoring system designed to quantify FCA progression and correlate with clinical outcomes. Methods- The VIPS study (Vascular Effects of Infection in Pediatric Stroke) prospectively enrolled 355 children with arterial ischemic stroke (2010-2014), including 41 with centrally confirmed FCA. Two neuroradiologists independently reviewed FCA cerebrovascular imaging, assigning a graded severity score of zero (no involvement) to 4 (occlusion) to individual arterial segments. The FCA severity score (FCASS) was the unweighted sum. In an iterative process, we modeled scores derived from different combinations of arterial segments to identify the model that optimized correlation with clinical outcome, simplicity, and reliability. Results- The optimal FCASS summed scores from 5 arterial segments: supraclinoid internal carotid artery, A1, A2, M1, and M2. The median (interquartile range) baseline FCASS was 4 (2-6). Of 33 children with follow-up imaging, the maximum FCASS (at any time point) was 7 (5-9). Twenty-four (73%) had FCA progression on follow-up with their maximum FCASS at a median of 8 (5-35.5) days poststroke; their median FCASS increase was 4 (2.5-6). FCASS did not correlate with recurrent arterial ischemic stroke. Maximum (but not baseline) FCASS correlated with 1-year pediatric stroke outcome measures ( P=0.037). Conclusions- Our novel scoring system for FCA severity correlates with neurological outcomes in the VIPS cohort and provides a tool for FCA treatment trials under development.
背景与目的-局灶性脑动脉病变(FCA)是既往健康儿童发生动脉缺血性脑卒中的常见原因,通常在数天至数周内进展,增加了再次发生脑卒中的风险。我们开发了一种新的严重程度评分系统,旨在量化 FCA 的进展并与临床结局相关联。
方法-VIPS 研究(儿科卒中感染的血管效应)前瞻性纳入了 355 例动脉缺血性脑卒中患儿(2010-2014 年),其中 41 例经中心确认存在 FCA。2 名神经放射科医生独立对 FCA 脑血管成像进行了评估,对各个动脉节段分别分配 0 级(无累及)至 4 级(闭塞)的分级严重程度评分。FCA 严重程度评分(FCASS)为无权重总和。在迭代过程中,我们对来自不同动脉节段组合的评分进行建模,以确定与临床结局相关性最佳、最简洁、最可靠的模型。
结果-最佳 FCASS 总分来自 5 个动脉节段:颈内动脉虹吸段、A1 段、A2 段、M1 段和 M2 段。基线 FCASS 的中位数(四分位距)为 4(2-6)。33 例有随访影像学的患儿中,最大 FCASS(任何时间点)为 7(5-9)。24 例(73%)在随访中有 FCA 进展,其最大 FCASS中位数为脑卒中后 8(5-35.5)天,FCASS 增加中位数为 4(2.5-6)。FCASS 与复发性动脉缺血性脑卒中无相关性。最大 FCASS(而非基线 FCASS)与 VIPS 队列中 1 年儿童脑卒中结局指标相关(P=0.037)。
结论-我们新的 FCA 严重程度评分系统与 VIPS 队列的神经结局相关,为正在开发的 FCA 治疗试验提供了一种工具。