Mungan İbrahim, Kazancı Dilek, Bektaş Şerife, Ademoglu Derya, Turan Sema
Department of Intensive Care Unit, Turkey Advanced Speciality Education and Research Hospital, Altındag, Ankara, Turkey.
BMC Anesthesiol. 2018 Oct 24;18(1):152. doi: 10.1186/s12871-018-0618-1.
ECMO support is a final treatment modality for patients in the refractory cardiogenic arrest and postcardiotomy cardiogenic shock with an utmost importance. Eventhough it is linked to high mortality, its usage gains popularity worldwide. We assessed the fluctuation of lactate levels and the clearance of lactate during the ECMO therapy and its prognostic role on mortality.
Data were gathered on all patients receiving ECMO therapy longer than 48 h between January 2015 and December 2017 retrospectively. Blood lactate had been recorded before ECMO implantation and at specific time points during ECMO support as a routine procedure. In this study, the Lactate clearance at specific time points (Lactate clearance-1) and the duration that lactate cleared more than 10% of the initial lactate level (Lactate clearance-2) was measured. Statistical analysis included Mann Whitney U-test and ROC-curves to predict 30-day mortality.
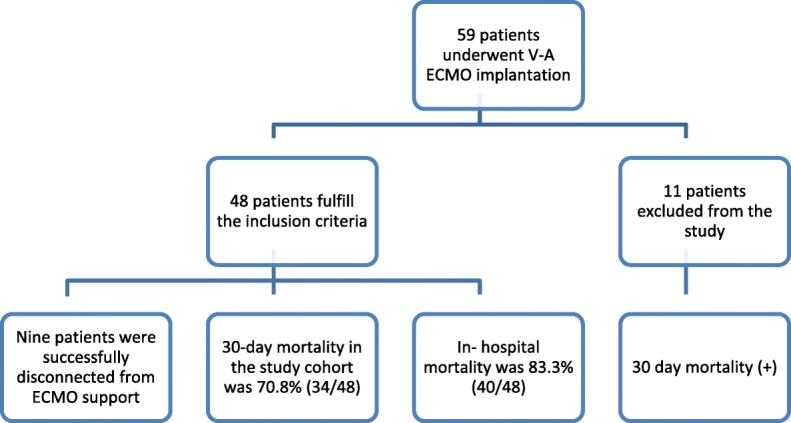
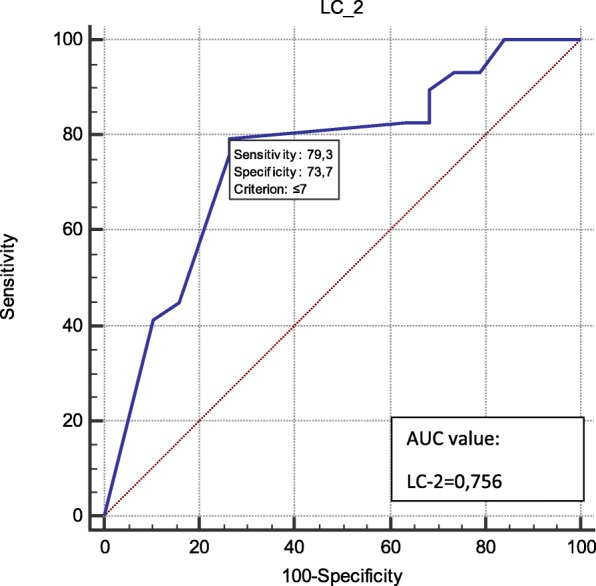
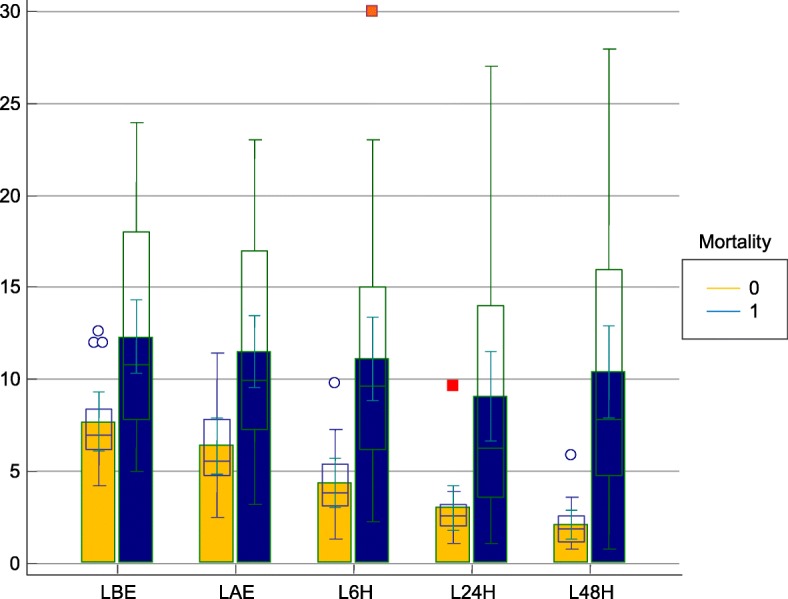
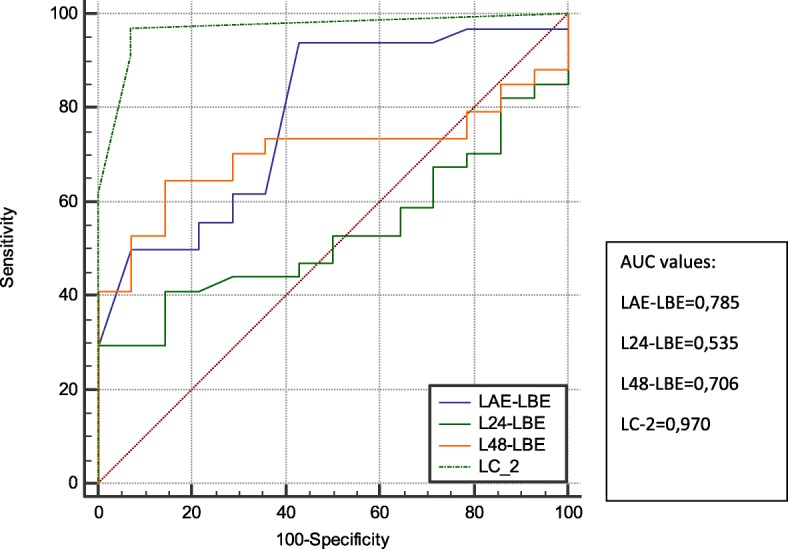
Fourty-eight patients underwent ECMO therapy for refractory cardiogenic shock resulting in 70.8% mortality. The lactate levels before and after ECMO therapy as well as the dynamic changes were significantly correlated with mortality variable. With AUC calculation, LC-2 has a strong discrimination (AUC = 0.97) on 30-day survivors and nonsurvivors. LAE-LBE (AUC = 0.785), L48-LBE (AUC = 0.706) showed moderate predictive power on 30-day mortality.
Changes in lactate levels after ECMO implantation is an important tool to assess effective circulatory support and it is found superior to single lactate measurements as a prognostic sign of mortality in our study. Based on our results, an early insertion of ECMO before lactate gets high was suggested. Serial changes on lactate levels and calculation of its clearance may be superior to single lactate on both effective circulatory support and as prognostic prediction. LC-2 showed a strong discrimination on 30-day mortality.
体外膜肺氧合(ECMO)支持是治疗难治性心源性骤停和心脏术后心源性休克患者的最终治疗方式,至关重要。尽管其与高死亡率相关,但其应用在全球范围内日益普遍。我们评估了ECMO治疗期间乳酸水平的波动及乳酸清除情况及其对死亡率的预后作用。
回顾性收集2015年1月至2017年12月期间所有接受ECMO治疗超过48小时的患者的数据。作为常规程序,在ECMO植入前及ECMO支持期间的特定时间点记录血乳酸。在本研究中,测量特定时间点的乳酸清除率(乳酸清除率-1)以及乳酸清除超过初始乳酸水平10%的持续时间(乳酸清除率-2)。统计分析包括Mann Whitney U检验和预测30天死亡率的ROC曲线。
48例患者因难治性心源性休克接受ECMO治疗,死亡率为70.8%。ECMO治疗前后的乳酸水平以及动态变化与死亡率变量显著相关。通过AUC计算,LC-2对30天存活者和非存活者有很强的鉴别力(AUC = 0.97)。LAE-LBE(AUC = 0.785)、L48-LBE(AUC = 0.706)对30天死亡率显示出中等预测能力。
ECMO植入后乳酸水平的变化是评估有效循环支持的重要工具,并且在我们的研究中发现其作为死亡率的预后指标优于单次乳酸测量。基于我们的结果,建议在乳酸水平升高之前尽早插入ECMO。乳酸水平的系列变化及其清除率的计算在有效循环支持和预后预测方面可能优于单次乳酸测量。LC-2对30天死亡率显示出很强的鉴别力。