Department of Health Policy Planning and Management, Makerere University School of Public Health, P.O Box 7072, Kampala, Uganda.
Department of Epidemiology and Biostatistics, School of Public Health, Makerere University College of Health Sciences, Kampala, Uganda.
BMC Infect Dis. 2018 Oct 24;18(1):533. doi: 10.1186/s12879-018-3450-9.
Lifelong antiretroviral therapy for HIV infected pregnant and lactating women (Option B+) has been rapidly scaled up but there are concerns about poor retention of women initiating treatment. However, facility-based data could underestimate retention in the absence of measures to account for self-transfers to other facilities. We assessed retention-in-care among women on Option B+ in Uganda, using facility data and follow-up to ascertain transfers to other facilities.
In a 25-month retrospective cohort analysis of routine program data, women who initiated Option B+ between March 2013 and March 2015 were tracked and interviewed quantitatively and qualitatively (in-depth interviews). Kaplan Meier survival analysis was used to estimate time to loss-to-follow-up (LTFU) while multivariable Cox proportional hazards regression was applied to estimate the adjusted predictors of LTFU, based on facility data. Thematic analysis was done for qualitative data, using MAXQDA 12. Quantitative data were analyzed with STATA® 13.
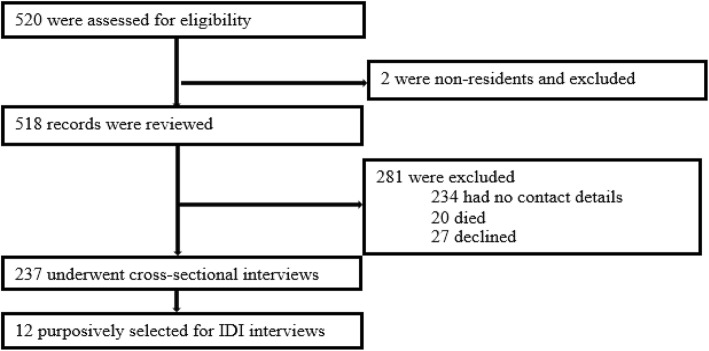
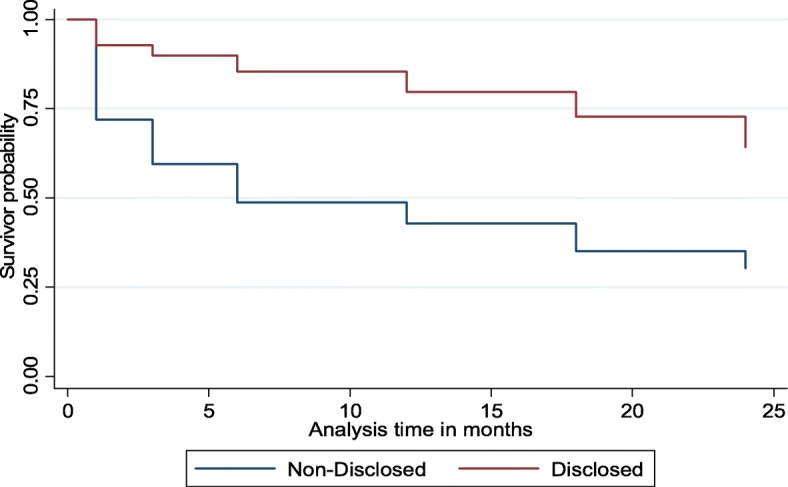
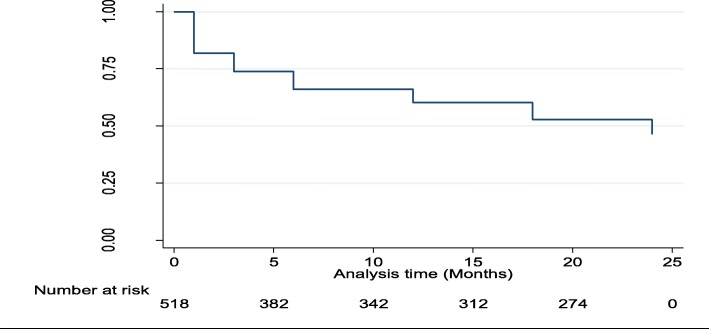
A total of 518 records were reviewed. The mean (SD) age was 26.4 (5.5) years, 289 women (55.6%) attended primary school, and 53% (276/518) had not disclosed their HIV status to their partners. At 25 months post-ART initiation, 278 (53.7%) were LTFU based on routine facility data, with mean time to LTFU of 15.6 months. Retention was 60.2 per 1000 months of observation (pmo) (95% CI: 55.9-64.3) at 12, and 46.3/1000pmo (95% CI: 42.0-50.5) at 25 months. Overall, 237 (55%) women were successfully tracked and interviewed and 43/118 (36.4%) of those who were classified as LTFU at facility level had self-transferred to another facility. The true 25 months post-ART initiation retention after tracking was 71.3% (169/237). Women < 25 years, aHR = 1.71 (95% CI: 1.28-2.30); those with no education, aHR = 5.55 (95% CI: 3.11-9.92), and those who had not disclosed their status to their partners, aHR = 1.59 (95% CI: 1.16-2.19) were more likely to be LTFU. Facilitators for Option B+ retention based on qualitative findings were adequate counselling, disclosure, and the desire to stay alive and raise HIV-free children. Drug side effects, inadequate counselling, stigma, and unsupportive spouses, were barriers to retention in care.
Retention under Option B+ is suboptimal and is under-estimated at health facility level. There is need to institute mechanisms for tracking of women across facilities. Retention could be enhanced through strategies to enhance disclosure to partners, targeting the uneducated, and those < 25 years.
为感染 HIV 的孕妇和哺乳期妇女提供终生抗逆转录病毒治疗(B 方案+)已迅速推广,但人们对开始治疗的妇女保留率低表示担忧。然而,如果没有考虑到将妇女转移到其他设施的措施,基于机构的数据可能会低估保留率。我们评估了乌干达 B 方案+中的妇女的护理保留率,使用机构数据和随访来确定转移到其他设施的情况。
在一项对常规方案数据的 25 个月回顾性队列分析中,跟踪并对 2013 年 3 月至 2015 年 3 月期间开始使用 B 方案+的妇女进行了定量和定性(深入访谈)采访。Kaplan-Meier 生存分析用于估计失访(LTFU)时间,而多变量 Cox 比例风险回归用于根据机构数据估计 LTFU 的调整预测因素。使用 MAXQDA 12 对定性数据进行主题分析,使用 STATA® 13 对定量数据进行分析。
共审查了 518 份记录。平均(SD)年龄为 26.4(5.5)岁,289 名妇女(55.6%)接受了小学教育,53%(276/518)未向其伴侣透露其 HIV 状况。在开始接受抗逆转录病毒治疗后 25 个月,根据常规机构数据,有 278 名(53.7%)妇女失访,平均失访时间为 15.6 个月。在 12 个月时,保留率为每 1000 个观察月 60.2(95%CI:55.9-64.3),在 25 个月时为 46.3/1000pmo(95%CI:42.0-50.5)。总体而言,有 237 名(55%)妇女成功接受了跟踪和采访,在机构层面被归类为失访的 43 名(118 名中的 36.4%)妇女已自行转移到另一家机构。经过跟踪后,抗逆转录病毒治疗后 25 个月的实际保留率为 71.3%(169/237)。年龄<25 岁的妇女,aHR=1.71(95%CI:1.28-2.30);未受过教育的妇女,aHR=5.55(95%CI:3.11-9.92);未向伴侣透露其状况的妇女,aHR=1.59(95%CI:1.16-2.19)更有可能失访。根据定性研究结果,B 方案+保留的促进因素包括充分的咨询、披露以及保持生存和生育无艾滋病毒子女的愿望。药物副作用、咨询不足、耻辱感和不支持的配偶是保留在护理中的障碍。
B 方案+的保留率不理想,在医疗机构层面被低估。有必要建立跟踪妇女在各机构之间的机制。通过增强与伴侣的披露、针对未受过教育的人和 25 岁以下的人等策略,保留率可以得到提高。