Mutiso Victoria N, Gitonga Isaiah, Musau Abednego, Musyimi Christine W, Nandoya Eric, Rebello Tahilia J, Pike Kathleen M, Ndetei David M
Africa Mental Health Research and Training Foundation, Matumbato Road, Off Elgon Road, Mawensi Gardens, Nairobi, Kenya.
2Global Mental Health Program, Columbia University, New York, USA.
Int J Ment Health Syst. 2018 Oct 15;12:57. doi: 10.1186/s13033-018-0234-y. eCollection 2018.
The World Health Organization developed the Mental Health Gap Action Programme Intervention Guide (mhGAP-IG) as guidelines for innovative utilization of available resources in low- and middle-income countries (LMICs) in order to accelerate the reduction of the mental health treatment gap. The mhGAP-IG calls for each country to contextualize the guide to their social, cultural and economic context. The objective of this paper is to describe a model for a stepwise approach for implementation of mhGAP-IG in a rural Kenyan setting using existing formal and informal community resources and health systems.
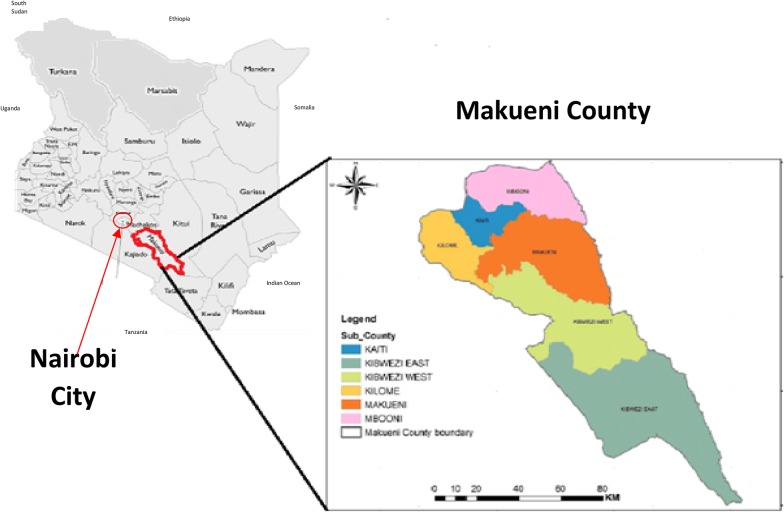
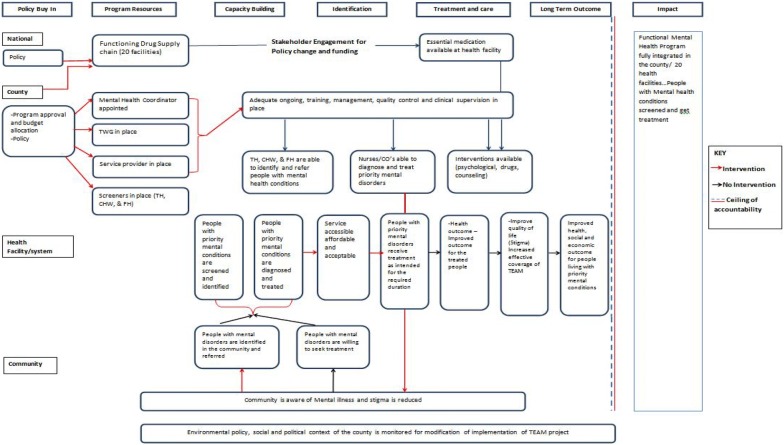
We conducted an analysis of mental health services in Makueni County, one of the 47 counties in Kenya, in order to understand the existing gaps and opportunities in a low-resource setting. We conducted stakeholder analysis and engagement through interactive dialogue in order for them to appreciate the importance of mental health to their communities. Through the process of participatory Theory of Change, the stakeholders gave their input on the process between the initiation and the end of the process for community mental health development, with the aim of achieving buy-in and collective ownership of the whole process. We adapted the mhGAP-IG to the local context and trained local human resources in skills necessary for the implementation of mhGAP-IG and for monitoring and evaluating the process using instruments with good psychometric properties that have been used in LMICs.
We were able to demonstrate the feasibility of implementing the mhGAP-IG using existing and trained community human resources using a multi-stakeholder approach. We further demonstrated the feasibility to transit seamlessly from research to policy and practice uptake using our approach.
An inclusive model for low resource settings is feasible and has the potential to bridge the gap between research, policy and practice. A major limitation of our study is that we did not engage a health economist from the beginning in order to determine the cost-effectiveness of our proposed model, occasioned by lack of resources to hire a suitable one.
世界卫生组织制定了《精神卫生差距行动计划干预指南》(mhGAP-IG),作为中低收入国家(LMICs)创新利用现有资源的指导方针,以加速缩小精神卫生治疗差距。mhGAP-IG要求每个国家根据其社会、文化和经济背景对该指南进行调整。本文的目的是描述一种在肯尼亚农村地区利用现有的正式和非正式社区资源及卫生系统逐步实施mhGAP-IG的模式。
我们对肯尼亚47个县之一的马库埃尼县的精神卫生服务进行了分析,以了解资源匮乏环境中现有的差距和机会。我们通过互动对话进行利益相关者分析和参与,以使他们认识到精神卫生对其社区的重要性。通过参与式变革理论过程,利益相关者就社区精神卫生发展过程从启动到结束的过程提供了意见,目的是实现对整个过程的认同和集体所有权。我们将mhGAP-IG调整为适应当地情况,并培训当地人力资源掌握实施mhGAP-IG以及使用中低收入国家已使用的具有良好心理测量特性的工具监测和评估该过程所需的技能。
我们能够证明使用多利益相关者方法利用现有和经过培训的社区人力资源实施mhGAP-IG的可行性。我们进一步证明了使用我们的方法从研究无缝过渡到政策和实践应用的可行性。
一种适用于资源匮乏环境的包容性模式是可行的,并且有可能弥合研究、政策和实践之间的差距。我们研究的一个主要局限性是,由于缺乏资源聘请合适的卫生经济学家,我们从一开始就没有让其参与以确定我们提议模式的成本效益。