Cha Teahyen, Choi Young Jin, Oh Jae-Won, Kim Chang-Ryul, Park Dong Woo, Seol In Joon, Moon Jin-Hwa
Department of Pediatrics, Hanyang University College of Medicine, Seoul, Korea.
Department of Radiology, Hanyang University Guri Hospital, Hanyang University College of Medicine, Guri, Korea.
Korean J Pediatr. 2019 Apr;62(4):131-137. doi: 10.3345/kjp.2018.07066. Epub 2018 Oct 23.
Respiratory syncytial virus (RSV) infection can cause various neurological complications. This study aimed to investigate the RSV-associated neurologic manifestations that present with seizures.
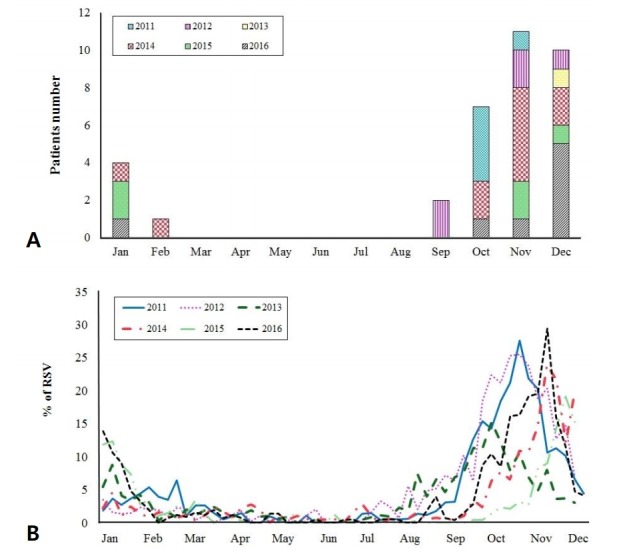
We retrospectively reviewed the medical records of patients aged less than 15 years with laboratory-confirmed RSV infections and seizures between January 2011 and December 2016 in a regional hospital in South Korea.
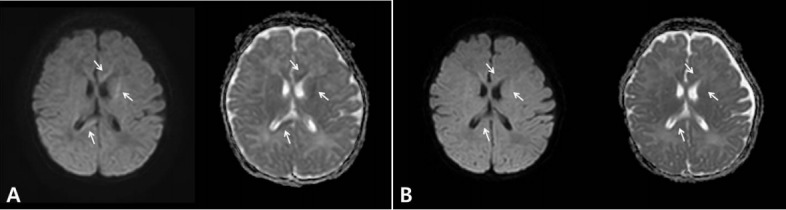
During this period, 1,193 patients with laboratory-confirmed RSV infection were identified. Of these, 35 (35 of 1,193, 2.93%; boys, 19; girls, 16; mean age: 20.8±16.6 months) presented with seizures. Febrile seizure was the most common diagnosis (27 of 35, 77.1%); simple febrile seizure in 13 patients (13 of 27, 48.1%) and complex febrile seizure in 14 (14 of 27, 51.9%). Afebrile seizures without meningitis or encephalopathy were observed in 5 patients (5 of 35, 14.3%), seizures with meningitis in 2 (2 of 35, 5.7%), and seizure with encephalopathy in 1 (1 of 35, 2.9%) patient. Lower respiratory symptoms were not observed in 8 patients. In a patient with encephalopathy, brain diffusion-weighted magnetic resonance imaging revealed transient changes in white matter, suggesting cytotoxic edema as the mechanism underlying encephalopathy. Most patients recovered with general management, and progression to epilepsy was noted in only 1 patient.
Although febrile seizure is the most common type of seizure associated with RSV infection, the proportion of patients with complex febrile seizure was higher than that of general febrile seizure. Transient cytotoxic edema may be a pathogenic mechanism in RSV-related encephalopathy with seizures.
呼吸道合胞病毒(RSV)感染可导致多种神经系统并发症。本研究旨在调查伴有癫痫发作的RSV相关神经表现。
我们回顾性分析了2011年1月至2016年12月期间韩国一家地区医院收治的年龄小于15岁、实验室确诊为RSV感染且伴有癫痫发作的患者的病历。
在此期间,共确定了1193例实验室确诊为RSV感染的患者。其中,35例(1193例中的35例,2.93%;男孩19例,女孩16例;平均年龄:20.8±16.6个月)出现癫痫发作。热性惊厥是最常见的诊断(35例中的27例,77.1%);单纯热性惊厥13例(27例中的13例,48.1%),复杂性热性惊厥14例(27例中的14例,51.9%)。5例患者(35例中的5例,14.3%)出现无脑膜炎或脑病的非热性惊厥,2例患者(35例中的2例,5.7%)出现伴有脑膜炎的惊厥,1例患者(35例中的1例,2.9%)出现伴有脑病的惊厥。8例患者未观察到下呼吸道症状。在1例患有脑病的患者中,脑部扩散加权磁共振成像显示白质有短暂变化,提示细胞毒性水肿是脑病的潜在机制。大多数患者通过一般治疗康复,仅1例患者进展为癫痫。
虽然热性惊厥是与RSV感染相关的最常见惊厥类型,但复杂性热性惊厥患者的比例高于一般热性惊厥患者。短暂性细胞毒性水肿可能是RSV相关脑病伴惊厥的发病机制。