Sherrod Brandon A, McClugage Samuel G, Mortellaro Vincent E, Aban Inmaculada B, Rocque Brandon G
Department of Neurosurgery, Division of Pediatric Neurosurgery, The University of Alabama at Birmingham and Children's Hospital of Alabama, Birmingham, AL.
Department of Neurosurgery, Division of Pediatric Neurosurgery, The University of Alabama at Birmingham and Children's Hospital of Alabama, Birmingham, AL.
J Pediatr Surg. 2019 Apr;54(4):631-639. doi: 10.1016/j.jpedsurg.2018.09.017. Epub 2018 Oct 10.
To evaluate venous thromboembolism (VTE) rates and risk factors following inpatient pediatric surgery.
153,220 inpatient pediatric surgical patients were selected from the 2012-2015 NSQIP-P database. Demographic and perioperative variables were documented. Primary outcome was VTE requiring treatment within 30 postoperative days. Secondary outcomes included length of stay (LOS) and 30-day mortality. Prediction models were generated using logistic regression. Mortality and time to VTE were assessed using Kaplan-Meier survival analysis.
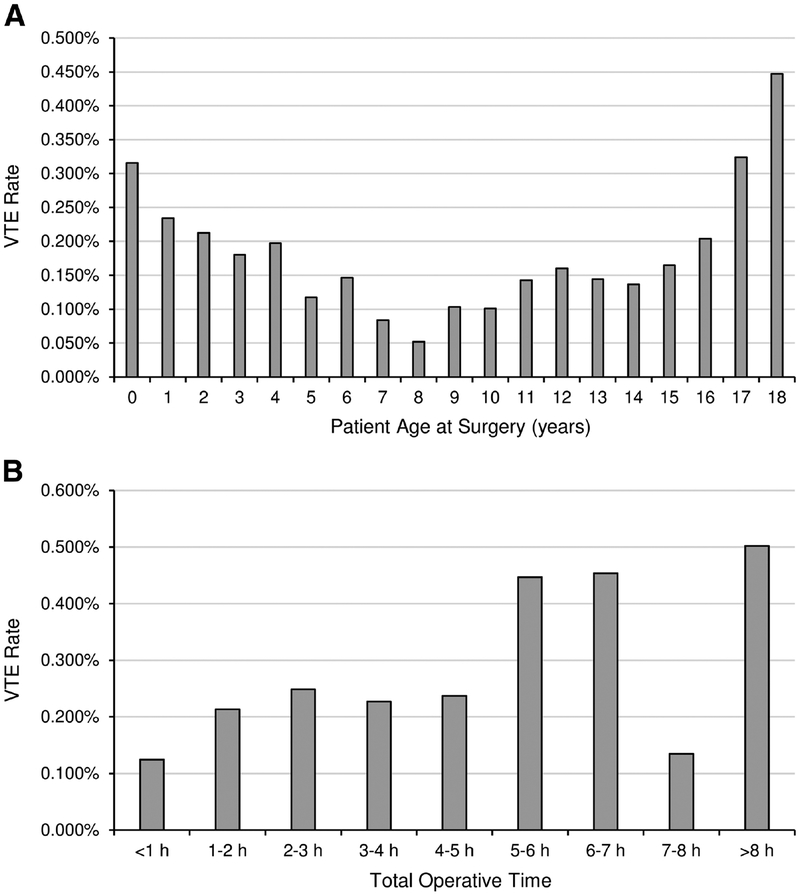
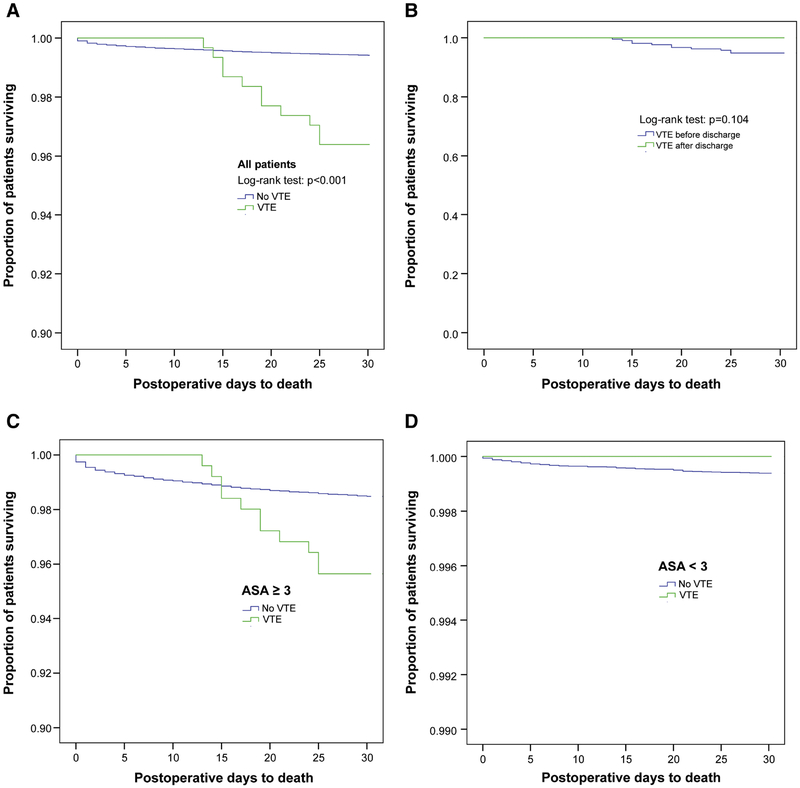
305 patients (0.20%) developed 296 venous thromboses and 12 pulmonary emboli (3 cooccurrences). Median time to VTE was 9 days. Most VTEs (81%) occurred predischarge. Subspecialties with highest VTE rates were cardiothoracic (0.72%) and general surgery (0.28%). No differences were seen for elective vs. urgent/emergent procedures (p = 0.106). All-cause mortality VTE patients was 1.2% vs. 0.2% in patients without VTE (p < 0.001). After stratifying by American Society of Anesthesiologists (ASA) class, no mortality differences remained when ASA < 3. Preoperative, postoperative, and total LOSs were longer for patients with VTE (p < 0.001 for each). ASA ≥ 3, preoperative sepsis, ventilator dependence, enteral/parenteral feeding, steroid use, preoperative blood transfusion, gastrointestinal disease, hematologic disorders, operative time, and age were independent predictors (C-statistic = 0.83).
Pediatric postsurgical patients have unique risk factors for developing VTE.
Level II.
评估小儿住院手术后静脉血栓栓塞症(VTE)的发生率及危险因素。
从2012 - 2015年NSQIP - P数据库中选取153,220例小儿住院手术患者。记录人口统计学和围手术期变量。主要结局是术后30天内需要治疗的VTE。次要结局包括住院时间(LOS)和30天死亡率。使用逻辑回归生成预测模型。使用Kaplan - Meier生存分析评估死亡率和VTE发生时间。
305例患者(0.20%)发生296例静脉血栓形成和12例肺栓塞(3例同时发生)。VTE的中位发生时间为9天。大多数VTE(81%)发生在出院前。VTE发生率最高的亚专业是心胸外科(0.72%)和普通外科(0.28%)。择期手术与急诊/紧急手术之间未见差异(p = 0.106)。VTE患者的全因死亡率为1.2%,无VTE患者为0.2%(p < 0.001)。按美国麻醉医师协会(ASA)分级分层后,当ASA < 3时,死亡率无差异。VTE患者的术前、术后及总住院时间更长(每项p < 0.001)。ASA≥3、术前脓毒症、呼吸机依赖、肠内/肠外营养、使用类固醇、术前输血、胃肠道疾病、血液系统疾病、手术时间和年龄是独立预测因素(C统计量 = 0.83)。
小儿术后患者发生VTE有独特危险因素。
二级。