Center for Respiratory Research and Rehabilitation, Department of Physical Therapy and McKnight Brain Institute, University of Florida, Gainesville, FL, USA.
J Cachexia Sarcopenia Muscle. 2019 Feb;10(1):63-72. doi: 10.1002/jcsm.12348. Epub 2018 Oct 25.
Cancer cachexia is an insidious process characterized by muscle atrophy with associated motor deficits, including diaphragm weakness and respiratory insufficiency. Although neuropathology contributes to muscle wasting and motor deficits in many clinical disorders, neural involvement in cachexia-linked respiratory insufficiency has not been explored.
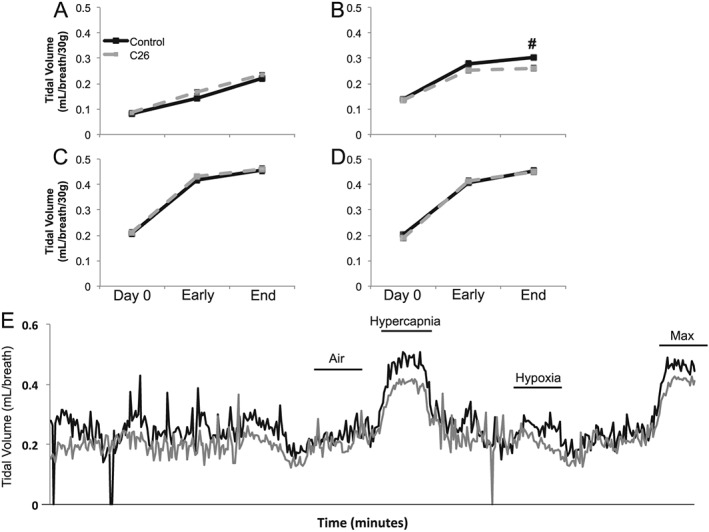
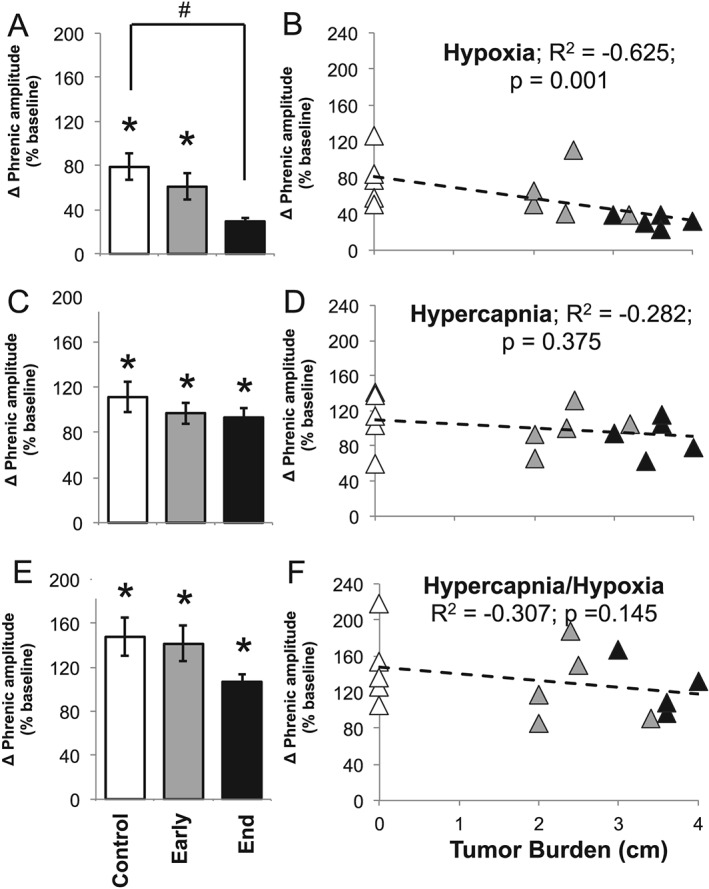
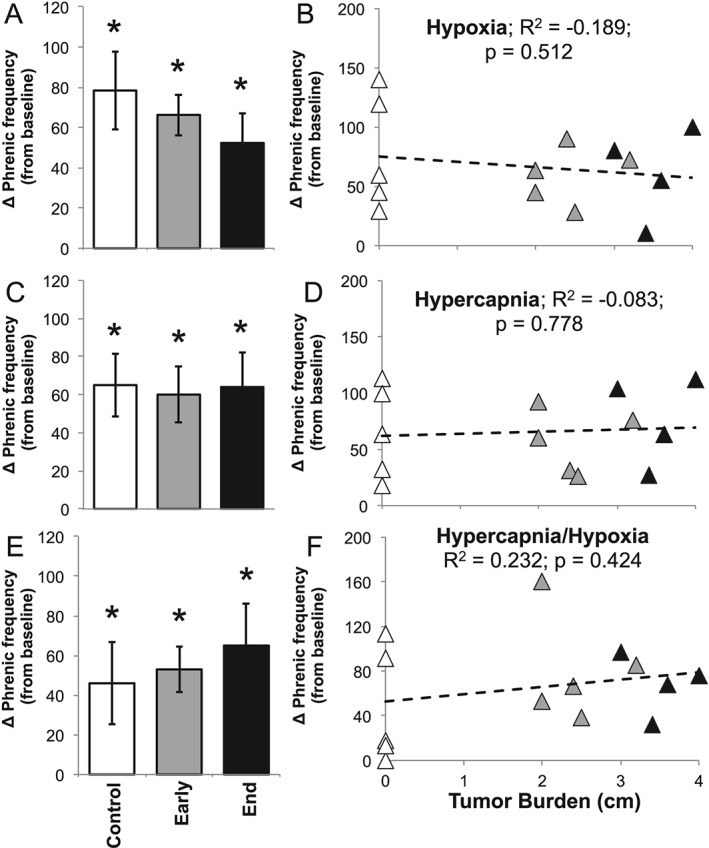
We first used whole-body plethysmography to assess ventilatory responses to hypoxic and hypercapnic chemoreflex activation in mice inoculated with the C26 colon adenocarcinoma cell line. Mice were exposed to a sequence of inspired gas mixtures consisting of (i) air, (ii) hypoxia (11% O ) with normocapnia, (iii) hypercapnia (7% CO ) with normoxia, and (iv) combined hypercapnia with hypoxia (i.e. maximal chemoreflex response). We also tested the respiratory neural network directly by recording inspiratory burst output from ligated phrenic nerves, thereby bypassing influences from changes in diaphragm muscle strength, respiratory mechanics, or compensation through recruitment of accessory motor pools.
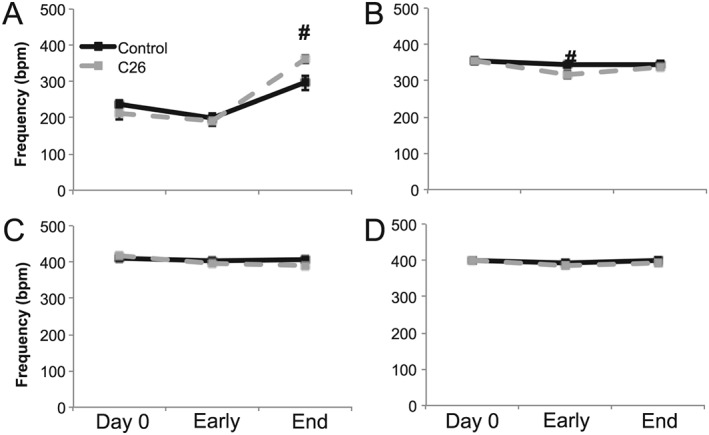
Cachectic mice demonstrated a significant attenuation of the hypoxic tidal volume (0.26mL±0.01mL vs 0.30mL±0.01mL; p<0.05), breathing frequency (317±10bpm vs 344±6bpm; p<0.05) and phrenic nerve (29.5±2.6% vs 78.8±11.8%; p<0.05) responses. On the other hand, the much larger hypercapnic tidal volume (0.46±0.01mL vs 0.46±0.01mL; p>0.05), breathing frequency (392±5bpm vs 408±5bpm; p>0.05) and phrenic nerve (93.1±8.8% vs 111.1±13.2%; p>0.05) responses were not affected. Further, the concurrent hypercapnia/hypoxia tidal volume (0.45±0.01mL vs 0.45±0.01mL; p>0.05), breathing frequency (395±7bpm vs 400±3bpm; p>0.05), and phrenic nerve (106.8±7.1% vs 147.5±38.8%; p>0.05) responses were not different between C26 cachectic and control mice.
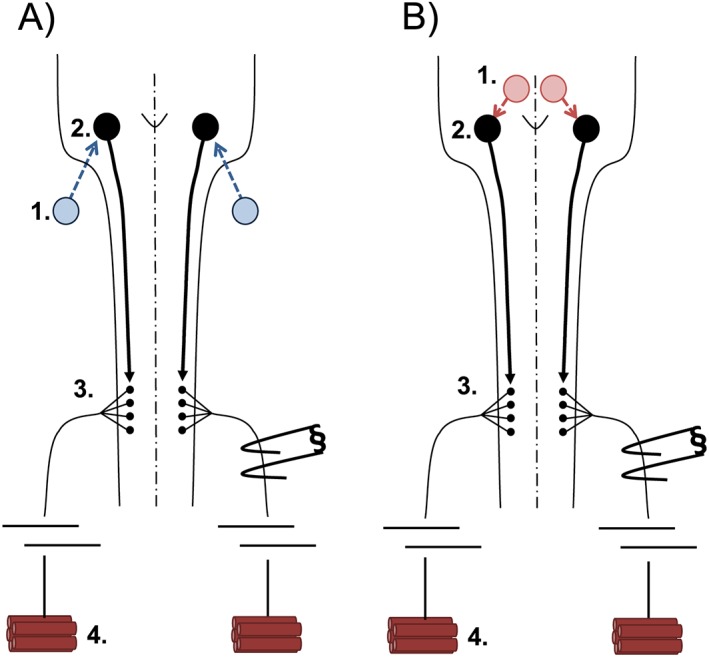
Breathing deficits associated with cancer cachexia are specific to the hypoxic ventilatory response and, thus, reflect disruptions in the hypoxic chemoafferent neural network. Diagnostic techniques that detect decompensation and therapeutic approaches that support the failing hypoxic respiratory response may benefit patients at risk for cancer cachectic-associated respiratory failure.
癌症恶病质是一种以肌肉萎缩为特征的隐匿性过程,伴有运动功能障碍,包括膈肌无力和呼吸功能不全。尽管神经病理学导致许多临床疾病中的肌肉消耗和运动功能障碍,但在与恶病质相关的呼吸功能不全中神经的参与尚未得到探索。
我们首先使用全身 plethysmography 来评估接种 C26 结肠腺癌细胞系的小鼠对缺氧和高碳酸血症化学感受器激活的通气反应。小鼠暴露于一系列吸入气体混合物中,包括 (i) 空气,(ii) 缺氧 (11% O2) 伴正常碳酸血症,(iii) 高碳酸血症 (7% CO2) 伴正常氧合,和 (iv) 高碳酸血症与缺氧联合 (即最大化学感受器反应)。我们还通过记录结扎膈神经的吸气爆发输出直接测试呼吸神经网络,从而绕过膈肌肌力、呼吸力学变化的影响,或通过募集辅助运动池来代偿。
恶病质小鼠的低氧潮气量 (0.26mL±0.01mL 对 0.30mL±0.01mL;p<0.05)、呼吸频率 (317±10bpm 对 344±6bpm;p<0.05) 和膈神经 (29.5±2.6% 对 78.8±11.8%;p<0.05) 反应明显减弱。另一方面,更大的高碳酸血症潮气量 (0.46±0.01mL 对 0.46±0.01mL;p>0.05)、呼吸频率 (392±5bpm 对 408±5bpm;p>0.05) 和膈神经 (93.1±8.8% 对 111.1±13.2%;p>0.05) 反应不受影响。此外,C26 恶病质和对照小鼠的同时高碳酸血症/缺氧潮气量 (0.45±0.01mL 对 0.45±0.01mL;p>0.05)、呼吸频率 (395±7bpm 对 400±3bpm;p>0.05) 和膈神经 (106.8±7.1% 对 147.5±38.8%;p>0.05) 反应没有差异。
与癌症恶病质相关的呼吸缺陷是特异性的缺氧通气反应,因此反映了缺氧化学感受器神经网络的中断。检测失代偿的诊断技术和支持衰竭的缺氧呼吸反应的治疗方法可能使癌症恶病质相关呼吸衰竭风险患者受益。