Anaesthesiology and Critical Care Department, Amiens University Hospital, Rond-point Fernand Leger, Amiens, France.
Anaesthesiology and Critical Care Department, Dijon University Hospital, 2 Bd Maréchal de Lattre de Tassigny, Dijon, France.
PLoS One. 2018 Oct 26;13(10):e0205950. doi: 10.1371/journal.pone.0205950. eCollection 2018.
The aim of the present study was to evaluate the ability of the ratios of central venous to arterial carbon dioxide content and tension to arteriovenous oxygen content to predict an increase in oxygen consumption (VO2) upon fluid challenge (FC).
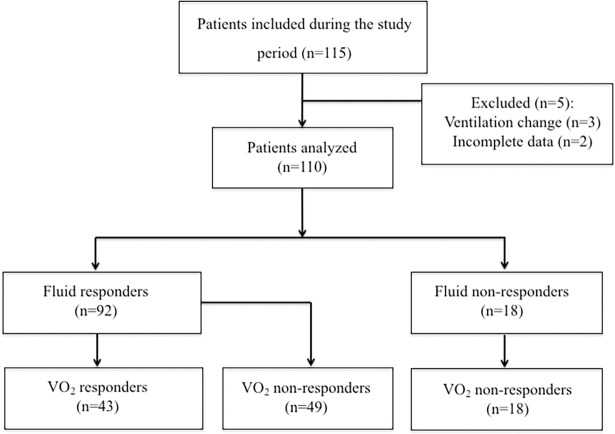
110 patients admitted to cardiothoracic ICU and in whom the physician had decided to perform an FC (with 500 ml of Ringer's lactate solution) were included. The arterial pressure, cardiac index (Ci), and arterial and venous blood gas levels were measured before and after FC. VO2 and CO2-O2 derived variables were calculated. VO2 responders were defined as patients showing more than a 15% increase in VO2. Of the 92 FC responders, 43 (46%) were VO2 responders. At baseline, pCO2 gap, C(a-v)O2 were lower in VO2 responders than in VO2 non-responders, and central venous oxygen saturation (ScvO2) was higher in VO2 responders. FC was associated with an increase in MAP, SV, and CI in both groups. With regard to ScvO2, FC was associated with an increase in VO2 non-responders and a decrease in VO2 responders. FC was associated with a decrease in pvCO2 and pCO2 gap in VO2 non-responders only. The pCO2 gap/C(a-v)O2 ratio and C(a-v)CO2 content /C(a-v)O2 content ratio did not change with FC. The CO2 gap content/C(a-v)O2 content ratio and the C(a-v)CO2 content /C(a-v)O2 content ratio did not predict fluid-induced VO2 changes (area under the curve (AUC) [95% confidence interval (CI)] = 0.52 [0.39‒0.64] and 0.53 [0.4-0.65], respectively; p = 0.757 and 0.71, respectively). ScvO2 predicted an increase of more than 15% in the VO2 (AUC [95%CI] = 0.67 [0.55‒0.78]; p<0.0001).
Our results showed that the ratios of central venous to arterial carbon dioxide content and tension to arteriovenous oxygen content were not predictive of VO2 changes following fluid challenge in postoperative cardiac surgery patients.
本研究旨在评估中心静脉与动脉二氧化碳含量和张力与动静脉氧含量比值预测液体冲击(FC)后氧耗(VO2)增加的能力。
纳入 110 例入住心胸 ICU 的患者,医生决定进行 FC(500ml 林格氏乳酸溶液)。在 FC 前后测量动脉压、心指数(Ci)和动脉及静脉血气水平。计算 VO2 和 CO2-O2 衍生变量。VO2 反应者定义为 VO2 增加超过 15%的患者。在 92 例 FC 反应者中,43 例(46%)为 VO2 反应者。在基线时,与 VO2 无反应者相比,pCO2 差、C(a-v)O2 更低,而 VO2 反应者的中心静脉血氧饱和度(ScvO2)更高。FC 后两组 MAP、SV 和 CI 均增加。就 ScvO2 而言,FC 后 VO2 无反应者增加,VO2 反应者减少。FC 后仅在 VO2 无反应者中 pvCO2 和 pCO2 差减少。只有在 VO2 无反应者中,pCO2 差/C(a-v)O2 比值和 C(a-v)CO2 含量/C(a-v)O2 含量比值随 FC 而变化。CO2 差含量/C(a-v)O2 含量比值和 C(a-v)CO2 含量/C(a-v)O2 含量比值不能预测液体诱导的 VO2 变化(曲线下面积(AUC)[95%置信区间(CI)]分别为 0.52[0.39-0.64]和 0.53[0.4-0.65];p=0.757 和 0.71,分别)。ScvO2 预测 VO2 增加超过 15%(AUC[95%CI] = 0.67[0.55-0.78];p<0.0001)。
我们的结果表明,中心静脉与动脉二氧化碳含量和张力与动静脉氧含量比值不能预测心脏手术后患者液体冲击后 VO2 的变化。